

Elevated T cell levels in peripheral blood predict poor clinical response following rituximab treatment in new-onset type 1 diabetes
- PMID: 29925930
- PMCID: PMC6477779
- DOI: 10.1038/s41435-018-0032-1
Elevated T cell levels in peripheral blood predict poor clinical response following rituximab treatment in new-onset type 1 diabetes
Abstract
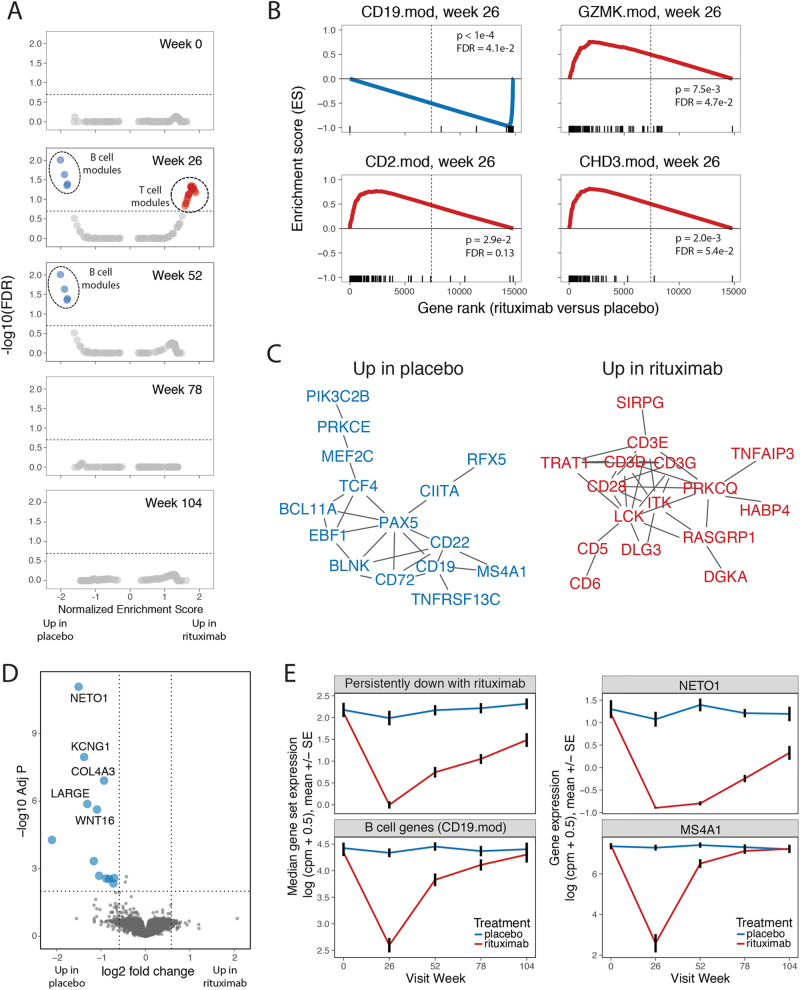
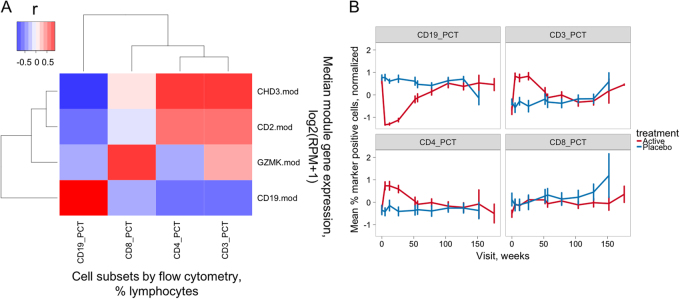
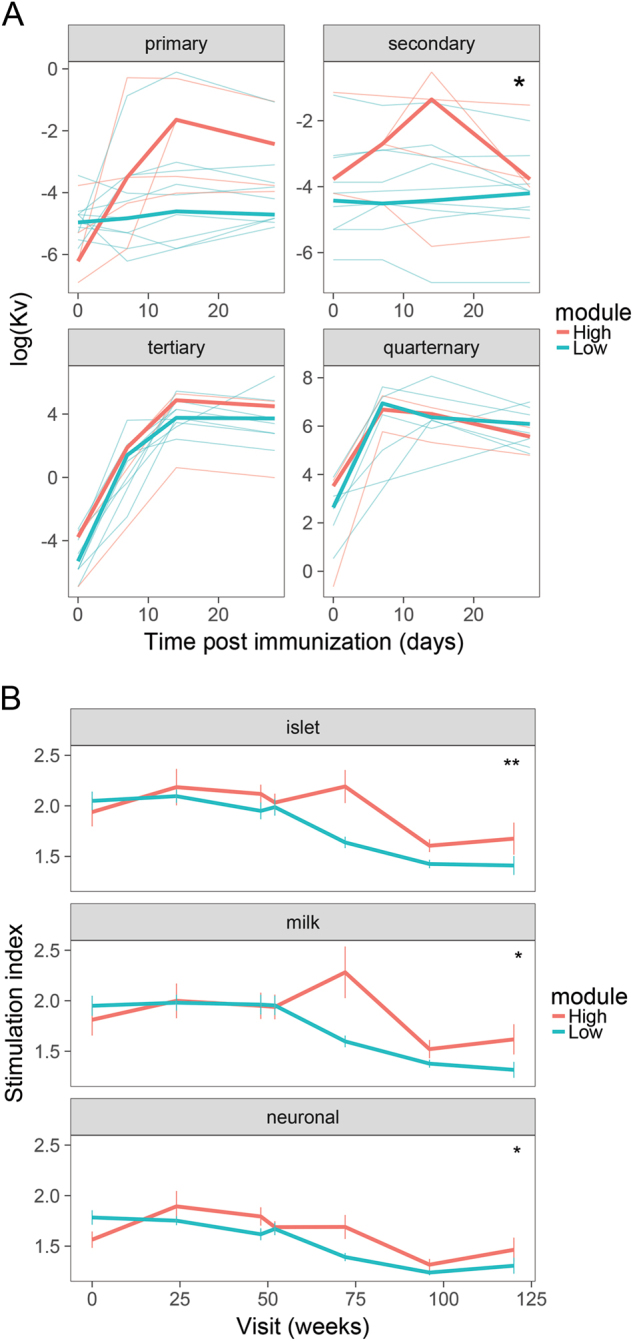
Biologic treatment of type 1 diabetes (T1D) with agents including anti-CD3 (otelixizumab and teplizumab), anti-CD20 (rituximab), LFA3Ig (alafacept), and CTLA4Ig (abatacept) results in transient stabilization of insulin C-peptide, a surrogate for endogenous insulin secretion. With the goal of inducing more robust immune tolerance, we used systems biology approaches to elucidate mechanisms associated with C-peptide stabilization in clinical trial blood samples from new-onset T1D subjects treated with the B cell-depleting drug, rituximab. RNA sequencing (RNA-seq) analysis of whole-blood samples from this trial revealed a transient increase in heterogeneous T cell populations, which were associated with decreased pharmacodynamic activity of rituximab, increased proliferative responses to islet antigens, and more rapid C-peptide loss. Our findings illustrate complexity in hematopoietic remodeling that accompanies B cell depletion by rituximab, which impacts and predicts therapeutic efficacy in T1D. Our data also suggest that a combination of rituximab with therapy targeting CD4 + T cells may be beneficial for T1D subjects.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- Herold KC, Gitelman SE, Ehlers MR, Gottlieb PA, Greenbaum CJ, Hagopian W, et al. Teplizumab (anti-CD3 mAb) treatment preserves C-peptide responses in patients with new-onset type 1 diabetes in a randomized controlled trial: metabolic and immunologic features at baseline identify a subgroup of responders. Diabetes. 2013;62:3766–74. doi: 10.2337/db13-0345. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 DK085476/DK/NIDDK NIH HHS/United States
- U01 DK061010/DK/NIDDK NIH HHS/United States
- UM1 AI109565/AI/NIAID NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U01 DK106993/DK/NIDDK NIH HHS/United States
- U01 DK103282/DK/NIDDK NIH HHS/United States
- UC4 DK106993/DK/NIDDK NIH HHS/United States
- U01 DK061042/DK/NIDDK NIH HHS/United States
- U01 DK085509/DK/NIDDK NIH HHS/United States
- UC4 DK117009/DK/NIDDK NIH HHS/United States
- P30 DK017047/DK/NIDDK NIH HHS/United States
- U01 DK085466/DK/NIDDK NIH HHS/United States
- U01 DK103153/DK/NIDDK NIH HHS/United States
- U01 DK061058/DK/NIDDK NIH HHS/United States
- U01 DK106984/DK/NIDDK NIH HHS/United States
- U01 DK085499/DK/NIDDK NIH HHS/United States
- U01 DK107013/DK/NIDDK NIH HHS/United States
- U01 DK103266/DK/NIDDK NIH HHS/United States
- U01 DK107014/DK/NIDDK NIH HHS/United States
- U01 DK106994/DK/NIDDK NIH HHS/United States
- U01 DK061034/DK/NIDDK NIH HHS/United States
- U01 DK085461/DK/NIDDK NIH HHS/United States
- DP3 DK104465/DK/NIDDK NIH HHS/United States
- U01 DK103180/DK/NIDDK NIH HHS/United States
- U01 DK085465/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
