

Assessment of Neurocognitive Functions in 7-Year-Old Children at Familial High Risk for Schizophrenia or Bipolar Disorder: The Danish High Risk and Resilience Study VIA 7
- PMID: 29926086
- PMCID: PMC6143091
- DOI: 10.1001/jamapsychiatry.2018.1415
Assessment of Neurocognitive Functions in 7-Year-Old Children at Familial High Risk for Schizophrenia or Bipolar Disorder: The Danish High Risk and Resilience Study VIA 7
Abstract
Importance: Children at familial high risk of schizophrenia spectrum disorders (FHR-SZ) or bipolar disorder (FHR-BP) exhibit neurocognitive impairments. Large studies of neurocognition in young children at familial high risk at the same age are important to differentiate the pathophysiology and developmental trajectory of these 2 groups.
Objective: To characterize neurocognitive functions in 7-year-old children with FHR-SZ or FHR-BP and a control population.
Design, setting, and participants: This multisite population-based cohort study collected data from January 1, 2013, to January 31, 2016, in the first wave of the Danish High Risk and Resilience Study VIA 7 at 2 university hospital research sites in Copenhagen and Aarhus using Danish registries. Participants (n = 514) included 197 children with FHR-SZ, 118 with FHR-BP, and 199 controls matched with the FHR-SZ group for age, sex, and municipality. Assessors were blinded to risk status.
Exposures: Parents with schizophrenia, bipolar disorder, or neither diagnosis.
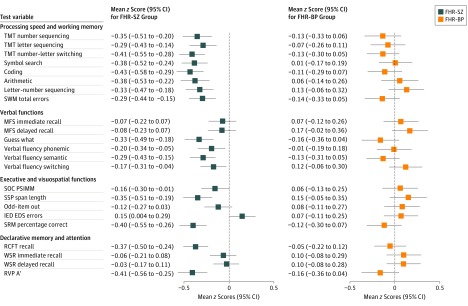
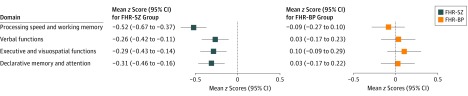
Main outcomes and measures: Neurocognitive functions were measured across 23 tests. Four neurocognitive domains were derived by principal component analysis, including processing speed and working memory, verbal functions, executive and visuospatial functions, and declarative memory and attention.
Results: A total of 514 children aged 7 years were included in the analysis (46.3% girls), consisting of 197 children with FHR-SZ (46.2% girls), 118 with FHR-BP (46.6% girls), and 199 controls (46.2% girls). Children with FHR-SZ were significantly impaired compared with controls on processing speed and working memory (Cohen d = 0.50; P < .001), executive and visuospatial functions (Cohen d = 0.28; P = .03), and declarative memory and attention (Cohen d = 0.29; P = .02). Compared with children with FHR-BP, children with FHR-SZ performed significantly poorer in processing speed and working memory (Cohen d = 0.40; P = .002), executive and visuospatial functions (Cohen d = 0.35; P = .008), and declarative memory and attention (Cohen d = 0.31; P = .03). Children with FHR-BP and controls did not differ.
Conclusions and relevance: Children with FHR-SZ had widespread neurocognitive impairments, supporting the hypothesis of neurocognitive functions as endophenotypes of schizophrenia. The absence of neurocognitive deficits in children with FHR-BP suggests distinct neurodevelopmental manifestations in these familial high-risk groups at this age. Early detection of children with FHR-SZ and cognitive impairments is warranted to investigate associations of neurocognition with transition to psychosis, add to the knowledge of their developmental pathophysiology, and inform early intervention programs.
Conflict of interest statement
Figures
References
-
- Weinberger DR. Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychiatry. 1987;44(7):660-669. - PubMed
-
- Rapoport JL, Addington AM, Frangou S, Psych MR. The neurodevelopmental model of schizophrenia: update 2005. Mol Psychiatry. 2005;10(5):434-449. - PubMed
-
- Trotta A, Murray RM, MacCabe JH. Do premorbid and post-onset cognitive functioning differ between schizophrenia and bipolar disorder? a systematic review and meta-analysis. Psychol Med. 2015;45(2):381-394. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
