

Prevalence of combined and noncombined dyslipidemia in an Iranian population
- PMID: 29926995
- PMCID: PMC6816872
- DOI: 10.1002/jcla.22579
Prevalence of combined and noncombined dyslipidemia in an Iranian population
Abstract
Background: Combination of dyslipidemic phenotypes, including elevated plasma levels of low-density lipoprotein cholesterol (LDL-C), elevated plasma triglycerides (TG), and decreased low-density lipoprotein cholesterol (HDL-C) concentrations, is important because of the association of individual phenotypes with increased risk of cardiovascular disease (CVD). We investigated the prevalence of combined dyslipidemias and their effects on CVD risk in an Iranian large population.
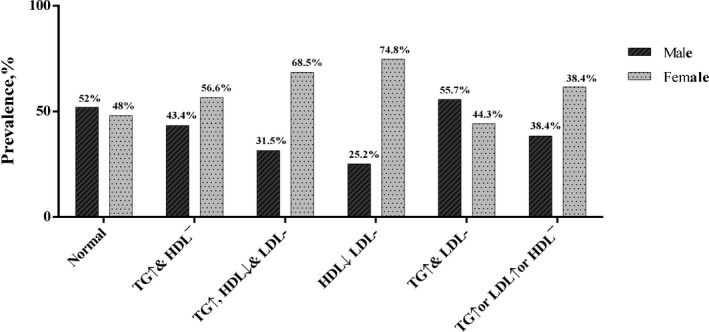
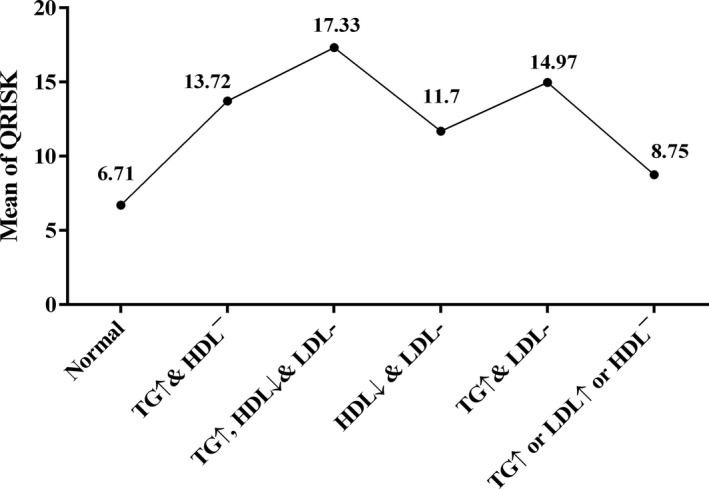
Method: A total of 9847 individuals were recruited as part of the Mashhad Stroke and Heart Atherosclerotic Disorders (MASHAD) cohort study. Anthropometric parameters and biochemical indices were measured in all of the subjects. Different types of combined dyslipidemias including high TG + low HDL-C, high TG + low HDL-C + high LDL-C, low HDL-C + high LDL-C, high TG + high LDL-C, and finally high TG + high LDL-C + low HDL-C were considered. Ten-year CVD risk was calculated using the QRISK2 risk algorithm and adjustments were made as suggested by the Joint British Societies' (JBS2). Logistic regression analyses were performed to determine the association between different combined dyslipidemias and categorical QRISK.
Results: A total of 3952 males and 5895 females were included in this current study. Among the included subjects, 83.4% had one form of dyslipidemia, and 16.6% subjects were not dyslipidemic. The mean age was 48.88 ± 7.9 and 47.02 ± 8.54 years for dyslipidemic and nondyslipidemic groups, respectively. The results showed that the frequency of dyslipidemia was 98%, 87.1%, and 90% in subjects with metabolic syndrome, CVD, and diabetes, respectively. Our results suggested that around 15.7% of study population were at 10 years CVD risk (high ≥20) and it was higher in men than women (P < .001). Moreover, risk of CVD was higher in TG↑ & HDL↓ & LDL↑ group than other groups.
Conclusion: Prevalence of dyslipidemia was 83.4% among Iranian adults. The results showed that individuals with increased plasma TG and LDL-C, and low HDL-C levels had the highest 10 years CVD risk compared to other combined dyslipidemic phenotypes.
Keywords: Iran; cardiovascular disease; diabetes mellitus; dyslipidemia.
© 2018 Wiley Periodicals, Inc.
Figures
Similar articles
-
Is Isolated Low High-Density Lipoprotein Cholesterol a Cardiovascular Disease Risk Factor? New Insights From the Framingham Offspring Study.Circ Cardiovasc Qual Outcomes. 2016 May;9(3):206-212. doi: 10.1161/CIRCOUTCOMES.115.002436. Epub 2016 May 10. Circ Cardiovasc Qual Outcomes. 2016. PMID: 27166203 Free PMC article.
-
Prevalence of dyslipidemia and associated risk factors among Turkish adults: Trabzon lipid study.Endocrine. 2008 Aug-Dec;34(1-3):36-51. doi: 10.1007/s12020-008-9100-z. Epub 2008 Nov 12. Endocrine. 2008. PMID: 19003544
-
[Analysis of dyslipidemia among patients with diabetes mellitus in Jilin Province communities].Wei Sheng Yan Jiu. 2014 Sep;43(5):743-8. Wei Sheng Yan Jiu. 2014. PMID: 25438527 Chinese.
-
Pathophysiology of Diabetic Dyslipidemia.J Atheroscler Thromb. 2018 Sep 1;25(9):771-782. doi: 10.5551/jat.RV17023. Epub 2018 Jul 12. J Atheroscler Thromb. 2018. PMID: 29998913 Free PMC article. Review.
-
Managing the residual cardiovascular disease risk associated with HDL-cholesterol and triglycerides in statin-treated patients: a clinical update.Nutr Metab Cardiovasc Dis. 2013 Sep;23(9):799-807. doi: 10.1016/j.numecd.2013.05.002. Epub 2013 Aug 9. Nutr Metab Cardiovasc Dis. 2013. PMID: 23932901 Review.
Cited by
-
Prevalence of dyslipidemia and its association with opium consumption in the Rafsanjan cohort study.Sci Rep. 2022 Jul 7;12(1):11504. doi: 10.1038/s41598-022-13926-3. Sci Rep. 2022. PMID: 35798768 Free PMC article.
-
Factors associated with dyslipidemia and its prevalence among Awash wine factory employees, Addis Ababa, Ethiopia: a cross-sectional study.BMC Cardiovasc Disord. 2022 Jan 30;22(1):22. doi: 10.1186/s12872-022-02465-4. BMC Cardiovasc Disord. 2022. PMID: 35094687 Free PMC article.
-
Associations Between Body Mass Index (BMI) and Dyslipidemia: Results From the PERSIAN Guilan Cohort Study (PGCS).Obes Sci Pract. 2025 Feb 6;11(1):e70055. doi: 10.1002/osp4.70055. eCollection 2025 Feb. Obes Sci Pract. 2025. PMID: 39917550 Free PMC article.
-
Pattern of dyslipidemia and associated factors in coronary artery disease patients in Khyber Pakhtunkhwa: A cross-sectional secondary data analysis.Pak J Med Sci. 2023 Sep-Oct;39(5):1416-1421. doi: 10.12669/pjms.39.5.7382. Pak J Med Sci. 2023. PMID: 37680793 Free PMC article.
-
Prevalence and 5-year incidence rate of dyslipidemia and its association with other coronary artery disease risk factors in Iran: Results of the Kerman coronary artery disease risk factors study (Phase 2).J Res Med Sci. 2021 Oct 18;26:99. doi: 10.4103/jrms.JRMS_748_20. eCollection 2021. J Res Med Sci. 2021. PMID: 34899937 Free PMC article.
References
-
- National Institutes of Health, National Heart Lung, Blood Institute . Atp iii guidelines at‐a‐glance quick desk reference. NIH publication 2001.
-
- Rizzo M, Barylski M, Rizvi AA, Montalto G, Mikhailidis DP, Banach M. Combined dyslipidemia: should the focus be ldl cholesterol or atherogenic dyslipidemia? Curr Pharm Des. 2013;19:3858‐3868. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
