

The influence of clinical, environmental, and socioeconomic factors on five-year patient survival after kidney transplantation
- PMID: 29927458
- PMCID: PMC6533991
- DOI: 10.1590/2175-8239-JBN-3865
The influence of clinical, environmental, and socioeconomic factors on five-year patient survival after kidney transplantation
Abstract
Introduction: The risk of death after kidney transplant is associated with the age of the recipient, presence of comorbidities, socioeconomic status, local environmental characteristics and access to health care.
Objective: To investigate the causes and risk factors associated with death during the first 5 years after kidney transplantation.
Methods: This was a single-center, retrospective, matched case-control study.
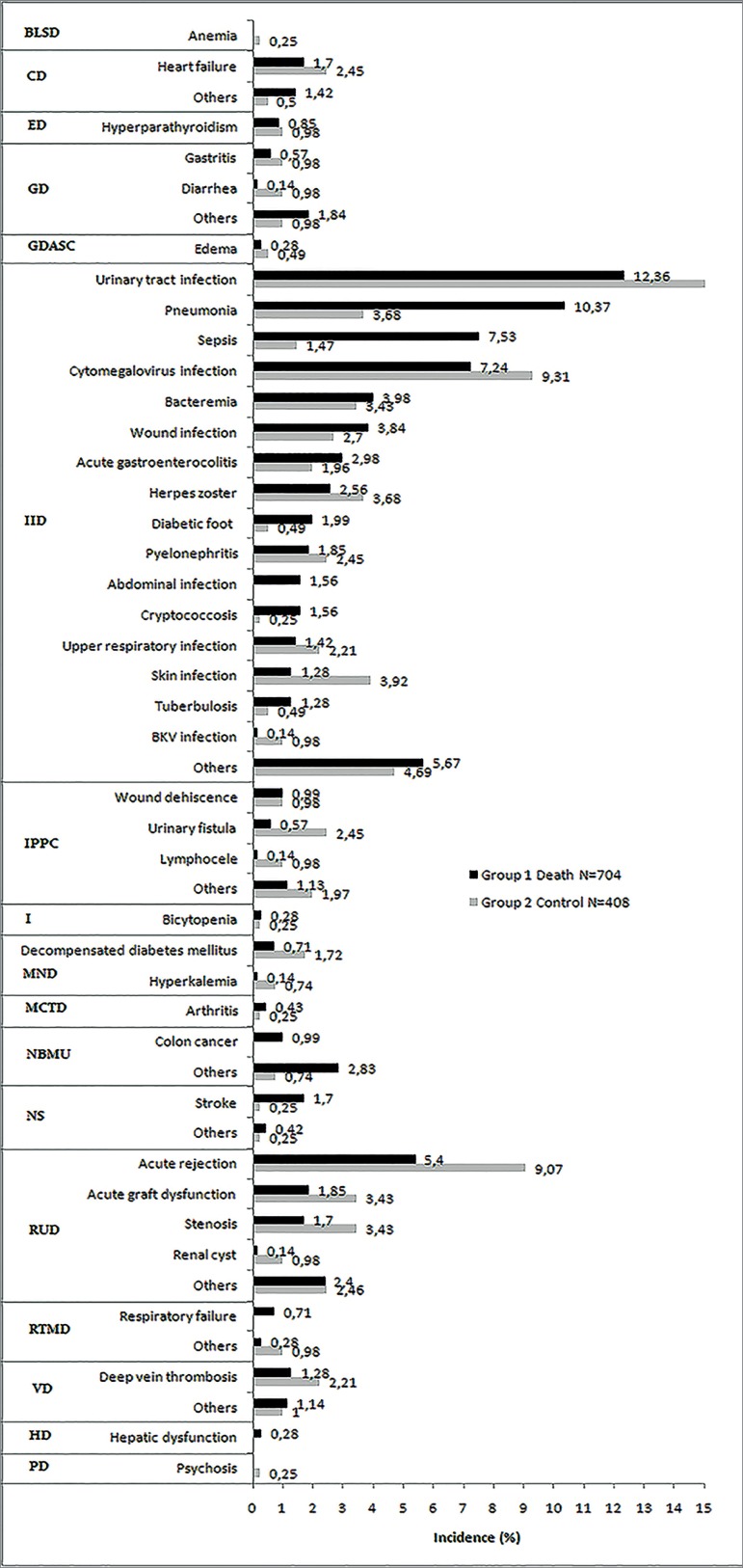
Results: Using a consecutive cohort of 1,873 kidney transplant recipients from January 1st 2007 to December 31st 2009, there were 162 deaths (case group), corresponding to 5-year patient survival of 91.4%. Of these deaths, 25% occurred during the first 3 months after transplant. The most prevalent cause of death was infectious (53%) followed by cardiovascular (24%). Risk factors associated with death were history of diabetes, dialysis type and time, unemployment, delayed graft function, number of visits to center, number of hospitalizations, and duration of hospital stay. After multivariate analysis, only time on dialysis, number of visits to center, and days in hospital were still associated with death. Patients who died had a non-significant higher number of treated acute rejection episodes (38% vs. 29%, p = 0.078), higher mean number of adverse events per patient (5.1 ± 3.8 vs. 3.8 ± 2.9, p = 0.194), and lower mean eGFR at 3 months (50.8 ± 25.1 vs. 56.7 ± 20.7, p = 0.137) and 48 months (45.9 ± 23.8 vs. 58.5 ± 20.2, p = 0.368).
Conclusion: This analysis confirmed that in this population, infection is the leading cause of mortality over the first 5 years after kidney transplantation. Several demographic and socioeconomic risk factors were associated with death, most of which are not readily modifiable.
Introdução:: O risco de óbito após transplante renal está associado à idade do receptor, presença de comorbidades, condição socioeconômica, às características ambientais locais e ao acesso a serviços de atenção à saúde.
Objetivo:: Investigar as causas e fatores de risco associados ao óbito nos primeiros cinco anos após o transplante renal.
Métodos:: Este é um estudo unicêntrico retrospectivo com pareamento dos grupos caso e controle.
Resultados:: Em uma coorte consecutiva de 1.873 receptores de transplante renal atendidos de 1/1/2007 a 31/12/2009 foram registrados 162 óbitos (grupo caso), correspondendo a uma taxa de sobrevida após cinco anos de 91,4%. Dos óbitos registrados, 25% ocorreram nos primeiros três meses após o transplante. A causa de óbito mais prevalente foi infecção (53%), seguida de doença cardiovascular (24%). Os fatores de risco associados a mortalidade foram histórico de diabetes, tipo e tempo em diálise, desemprego, função tardia do enxerto, número de consultas, número de hospitalizações e tempo de internação hospitalar. Após análise multivariada, apenas o tempo em diálise, o número de consultas e dias de internação permaneceram associados a mortalidade. Os pacientes que foram a óbito tiveram um número não significativamente maior de tratamentos de episódios de rejeição aguda (38% vs. 29%; p = 0,078), maior número médio de eventos adversos por paciente (5,1 ± 3,8 vs. 3,8 ± 2,9; p = 0,194) e TFGe média mais baixa aos três meses (50,8 ± 25,1 vs. 56,7 ± 20,7; p = 0,137) e 48 meses (45,9 ± 23,8 vs. 58,5 ± 20,2; p = 0,368).
Conclusão:: A presente análise confirmou que nessa população, a infecção foi a principal causa de mortalidade nos primeiros cinco anos após transplante renal. Vários fatores de risco demográficos e socioeconômicos foram associados a mortalidade, a maioria não prontamente modificável.
Figures
References
-
- de Castro Rodrigues Ferreira F, Cristelli MP, Paula MI, Proença H, Felipe CR, Tedesco-Silva H, et al. Infectious complications as the leading cause of death after kidney transplantation: analysis of more than 10,000 transplants from a single center. J Nephrol. 2017;30:601–606. - PubMed
-
- Karim A, Farrugia D, Cheshire J, Mahboob S, Begaj I, Ray D, et al. Recipient age and risk for mortality after kidney transplantation in England. Transplantation. 2014;97:832–838. - PubMed
-
- Gusukuma LW, Silva HT, Jr, Pestana JO. Risk assessment score in pre-kidney transplantation: methodology and the socioeconomic characteristics importance. J Bras Nefrol. 2014;36:339–351. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
