

The currency, completeness and quality of systematic reviews of acute management of moderate to severe traumatic brain injury: A comprehensive evidence map
- PMID: 29927963
- PMCID: PMC6013193
- DOI: 10.1371/journal.pone.0198676
The currency, completeness and quality of systematic reviews of acute management of moderate to severe traumatic brain injury: A comprehensive evidence map
Abstract
Objective: To appraise the currency, completeness and quality of evidence from systematic reviews (SRs) of acute management of moderate to severe traumatic brain injury (TBI).
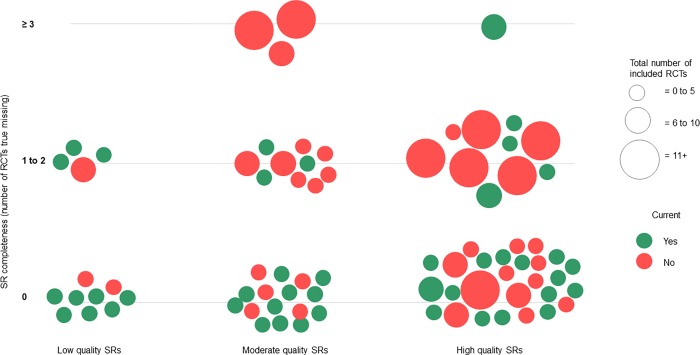
Methods: We conducted comprehensive searches to March 2016 for published, English-language SRs and RCTs of acute management of moderate to severe TBI. Systematic reviews and RCTs were grouped under 12 broad intervention categories. For each review, we mapped the included and non-included RCTs, noting the reasons why RCTs were omitted. An SR was judged as 'current' when it included the most recently published RCT we found on their topic, and 'complete' when it included every RCT we found that met its inclusion criteria, taking account of when the review was conducted. Quality was assessed using the AMSTAR checklist (trichotomised into low, moderate and high quality).
Findings: We included 85 SRs and 213 RCTs examining the effectiveness of treatments for acute management of moderate to severe TBI. The most frequently reviewed interventions were hypothermia (n = 17, 14.2%), hypertonic saline and/or mannitol (n = 9, 7.5%) and surgery (n = 8, 6.7%). Of the 80 single-intervention SRs, approximately half (n = 44, 55%) were judged as current and two-thirds (n = 52, 65.0%) as complete. When considering only the most recently published review on each intervention (n = 25), currency increased to 72.0% (n = 18). Less than half of the 85 SRs were judged as high quality (n = 38, 44.7%), and nearly 20% were low quality (n = 16, 18.8%). Only 16 (20.0%) of the single-intervention reviews (and none of the five multi-intervention reviews) were judged as current, complete and high-quality. These included reviews of red blood cell transfusion, hypothermia, management guided by intracranial pressure, pharmacological agents (various) and prehospital intubation. Over three-quarters (n = 167, 78.4%) of the 213 RCTs were included in one or more SR. Of the remainder, 17 (8.0%) RCTs post-dated or were out of scope of existing SRs, and 29 (13.6%) were on interventions that have not been assessed in SRs.
Conclusion: A substantial number of SRs in acute management of moderate to severe TBI lack currency, completeness and quality. We have identified both potential evidence gaps and also substantial research waste. Novel review methods, such as Living Systematic Reviews, may ameliorate these shortcomings and enhance utility and reliability of the evidence underpinning clinical care.
Conflict of interest statement
We have read the journal's policy and the authors of this manuscript have the following competing interests: AS, CL and ED are employed by or affiliated with Cochrane Australia, Monash University. Cochrane Australia is part of Cochrane, a not-for-profit organisation and global independent network of researchers, professionals, patients, carers and people interested in health, who publish and promote systematic reviews. The authors of this evidence map did not author any of the included systematic reviews. Neither Cochrane Australia, Cochrane nor the authors stand to gain any financial benefit from the results of this study. This does not alter our adherence to PLOS ONE policies on sharing data and material.
Figures
Similar articles
-
An overview of systematic reviews on the pharmacological randomized controlled trials for reducing intracranial pressure after traumatic brain injury.Brain Inj. 2022 Jun 7;36(7):829-840. doi: 10.1080/02699052.2022.2087102. Epub 2022 Jun 16. Brain Inj. 2022. PMID: 35708261 Review.
-
Overview of pharmacological interventions after traumatic brain injuries: impact on selected outcomes.Brain Inj. 2019;33(4):442-455. doi: 10.1080/02699052.2019.1565896. Epub 2019 Jan 29. Brain Inj. 2019. PMID: 30694081 Review.
-
Hypertonic saline versus other intracranial pressure-lowering agents for people with acute traumatic brain injury.Cochrane Database Syst Rev. 2020 Jan 17;1(1):CD010904. doi: 10.1002/14651858.CD010904.pub3. Cochrane Database Syst Rev. 2020. PMID: 31978260 Free PMC article.
-
A State-of-the-Science Overview of Randomized Controlled Trials Evaluating Acute Management of Moderate-to-Severe Traumatic Brain Injury.J Neurotrauma. 2016 Aug 15;33(16):1461-78. doi: 10.1089/neu.2015.4233. Epub 2016 Mar 18. J Neurotrauma. 2016. PMID: 26711675 Free PMC article. Review.
-
Interventions for patent ductus arteriosus (PDA) in preterm infants: an overview of Cochrane Systematic Reviews.Cochrane Database Syst Rev. 2023 Apr 11;4(4):CD013588. doi: 10.1002/14651858.CD013588.pub2. Cochrane Database Syst Rev. 2023. PMID: 37039501 Free PMC article. Review.
Cited by
-
Systematic reviews on platelet transfusions: Is there unnecessary duplication of effort? A scoping review.Vox Sang. 2023 Jan;118(1):16-23. doi: 10.1111/vox.13387. Epub 2022 Dec 1. Vox Sang. 2023. PMID: 36454598 Free PMC article.
-
Low-value clinical practices in adult traumatic brain injury: an umbrella review protocol.BMJ Open. 2019 Oct 9;9(10):e031747. doi: 10.1136/bmjopen-2019-031747. BMJ Open. 2019. PMID: 31601599 Free PMC article.
-
Characteristics and Impact of U.S. Military Blast-Related Mild Traumatic Brain Injury: A Systematic Review.Front Neurol. 2020 Nov 2;11:559318. doi: 10.3389/fneur.2020.559318. eCollection 2020. Front Neurol. 2020. PMID: 33224086 Free PMC article.
-
A living critical interpretive synthesis to yield a framework on the production and dissemination of living evidence syntheses for decision-making.Implement Sci. 2024 Sep 27;19(1):67. doi: 10.1186/s13012-024-01396-2. Implement Sci. 2024. PMID: 39334425 Free PMC article. Review.
-
An Overview of Randomized Controlled Trials Examining Prescription and Nonprescription Pharmacological Interventions for Moderate to Severe Traumatic Brain Injury.J Pharm Technol. 2024 Nov 16:87551225241296420. doi: 10.1177/87551225241296420. Online ahead of print. J Pharm Technol. 2024. PMID: 39564452 Free PMC article. Review.
References
-
- Institute of Medicine. Institute of Medicine (US) Committee on Standards for Systematic Reviews of Comparative Effectiveness Research Eden J, Levit L, Berg A, Morton S, editors. Washington (DC): National Academies Press (US); 2011. - PubMed
-
- Oxman AD, Cook DJ, Guyatt GH. Users' guides to the medical literature. VI. How to use an overview. Evidence-Based Medicine Working Group. Jama. 1994;272(17):1367–71. - PubMed
-
- Institute of Medicine. Current Best Practices and Proposed Standards for Development of Trustworthy CPGs: Part 1, Getting Started In: Robin Graham MM, Wolman Dianne Miller, Greenfield Sheldon, and Steinberg Earl, editor. Clinical practice guidelines we can trust Washington DC: Institute of Medicine; 2011. p. 75–108.
-
- Robinson KA, Saldanha IJ, McKoy NA. Development of a framework to identify research gaps from systematic reviews. Journal of clinical epidemiology. 2011;64(12):1325–30. doi: 10.1016/j.jclinepi.2011.06.009 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
