

Reconstruction of Type II abdominal wall defects: Anterolateral thigh or tensor fascia lata myocutaneous flaps?
- PMID: 29928077
- PMCID: PMC5992935
- DOI: 10.4103/ijps.IJPS_75_15
Reconstruction of Type II abdominal wall defects: Anterolateral thigh or tensor fascia lata myocutaneous flaps?
Abstract
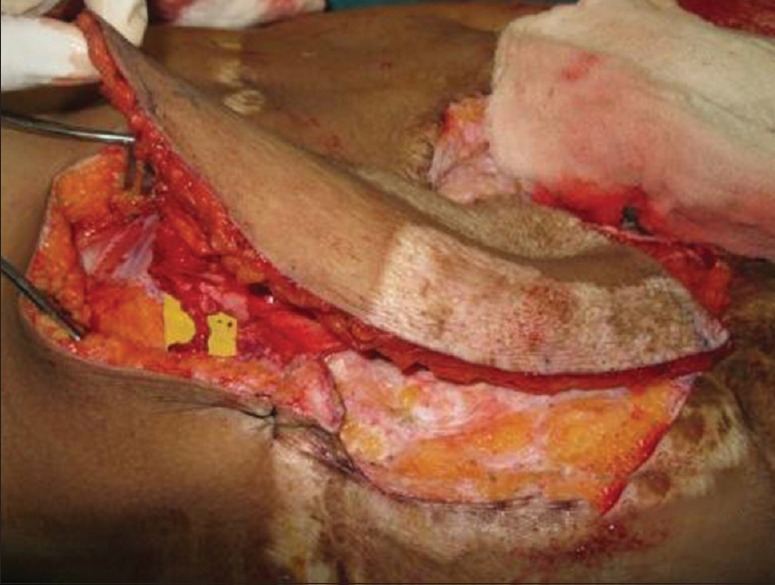
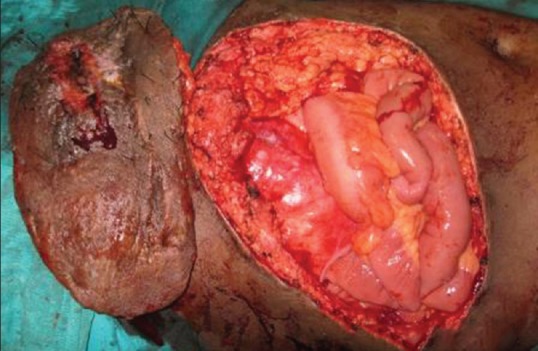
Introduction: Reconstruction of complex abdominal wall defects is both challenging and technically demanding for plastic surgeon. Objectives in abdominal wall reconstruction are consistent and include restoration of abdominal wall integrity, protection of intra abdominal viscera and prevention of herniation.
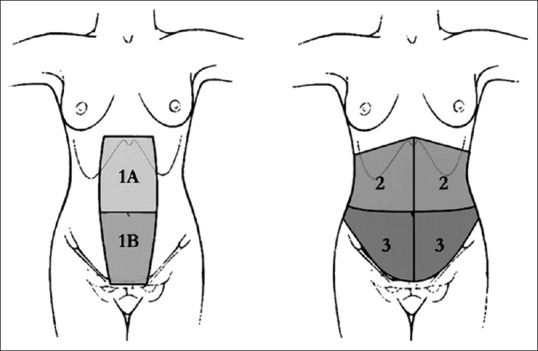
Materials: We conducted a retrospective study on five patients in whom lateral thigh flaps such as anterolateral thigh (ALT) flaps and tensor fascia lata (TFL) myocutaneous flaps as pedicled or free flaps were used for complex abdominal wall Type II defects over a 5- years period between 2007 and 2012.
Results: In two patients, free flaps were used for reconstruction of the upper abdomen and both were ALT. In three patients of lower abdominal defects, one patient had bilateral pedicled ALT flaps, one pedicled TFL myocutaneous and one free TFL myocutaneous in view of ipsilateral electric burn scars. There were no flap losses. Patients were followed up beyond 6 months and found to have a good abdominal contour and only one of five had clinical evidence of herniation.
Conclusion: It can be concluded that flap from the Lateral thigh (ALT or TFL) is flap of choice for large Type II abdominal defects. Including vascularised fascia in the flap maintains abdominal wall integrity and use of synthetic mesh is not necessary. Upper abdominal defects need free flaps and in lower abdominal defects a pedicled flap suffices.
Keywords: Complex anterior abdominal wall defects; pedicle and free anterolateral thigh flaps and Tensor Fascia Lata Flap; reconstruction; vascularised fascia.
Conflict of interest statement
There are no conflicts of interest.
Figures








References
-
- Read RR. Ventral, epigastric, umbilical, spigelian and incisional hernias. In: Cameron JL, editor. Current Surgical Therapy. 5th ed. Philadelphia: Mosby; 1995. pp. 491–6.
-
- Larson GM, Vandertoll DJ. Approaches to repair of ventral hernia and full-thickness losses of the abdominal wall. Surg Clin North Am. 1984;64:335–49. - PubMed
-
- Hurwotz DJ, Hollins RR. Reconstruction of the abdominal wall and groin. In: Cohen M, editor. Mastery of Plastic and Reconstructive Surgery. Boston: Little, Brown; 1994. pp. 1349–59.
-
- Tukiainen E, Leppäniemi A. Reconstruction of extensive abdominal wall defects with microvascular tensor fasciae latae flap. Br J Surg. 2011;98:880–4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources