

Neurological Disease in Lupus: Toward a Personalized Medicine Approach
- PMID: 29928273
- PMCID: PMC5997834
- DOI: 10.3389/fimmu.2018.01146
Neurological Disease in Lupus: Toward a Personalized Medicine Approach
Abstract
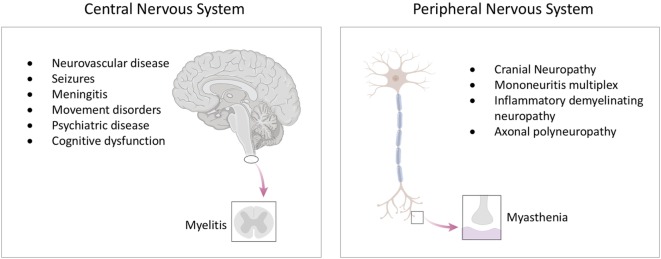
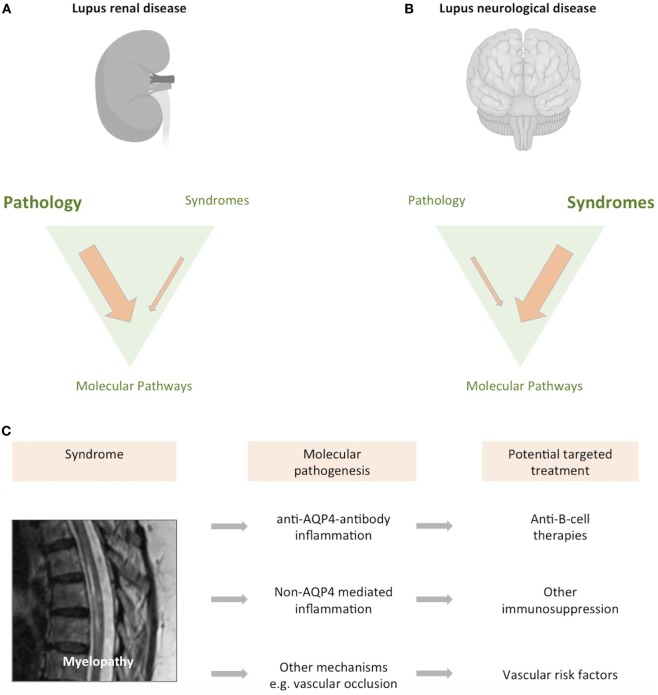
The brain and nervous system are important targets for immune-mediated damage in systemic lupus erythematosus (SLE), resulting in a complex spectrum of neurological syndromes. Defining nervous system disease in lupus poses significant challenges. Among the difficulties to be addressed are a diversity of clinical manifestations and a lack of understanding of their mechanistic basis. However, despite these challenges, progress has been made in the identification of pathways which contribute to neurological disease in SLE. Understanding the molecular pathogenesis of neurological disease in lupus will inform both classification and approaches to clinical trials.
Keywords: interferon type I; lupus erythematosus; neurolupus; personalized medicine; systemic; targeted therapy.
Figures

References
-
- Kaposi M. Lupus erythematosus. In: Hebra H, Kaposi M, editors. Diseases of the Skin Including the Exanthemata. Vol IV. 1875 London: The New Sydenham Society; (1880), p. 14–37. (transl. By Tay W).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases