

Liquid biopsy in pancreatic cancer: the beginning of a new era
- PMID: 29928492
- PMCID: PMC6003564
- DOI: 10.18632/oncotarget.24809
Liquid biopsy in pancreatic cancer: the beginning of a new era
Abstract
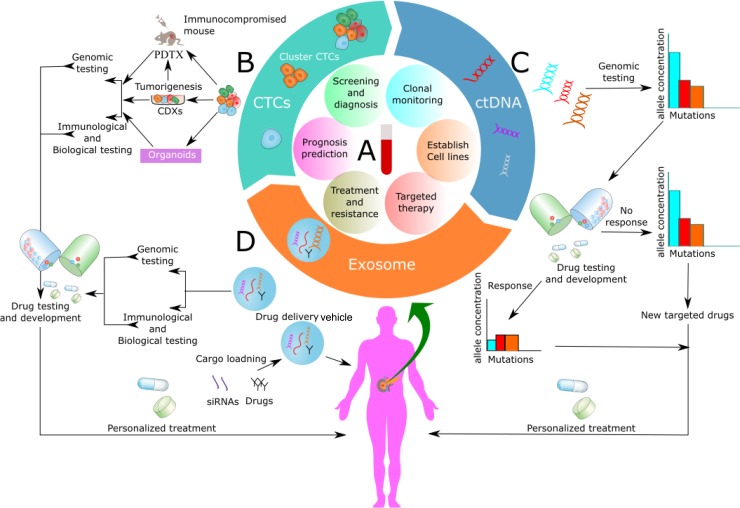
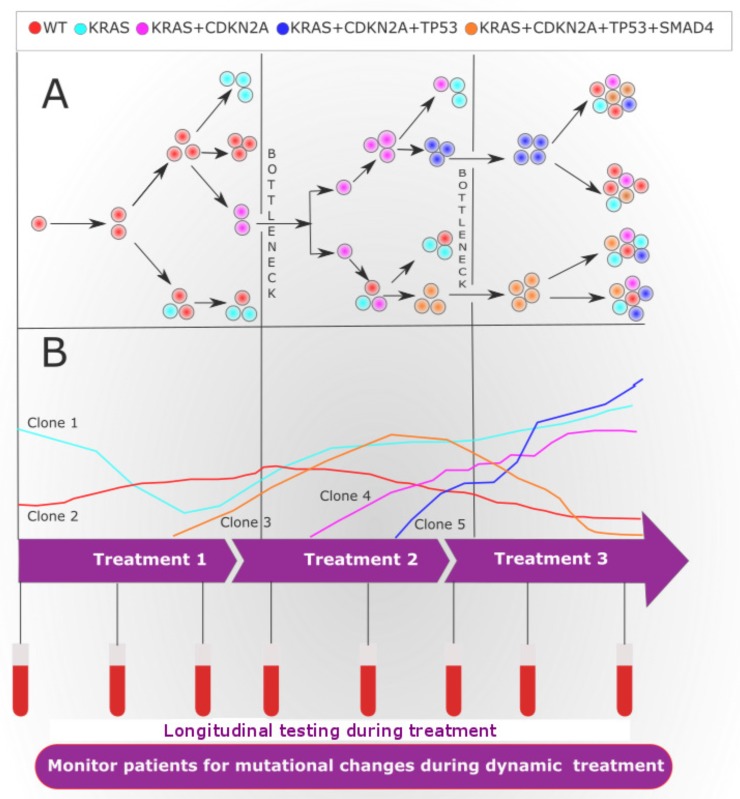
With dismal survival rate pancreatic cancer remains one of the most aggressive and devastating malignancy. Predominantly, due to the absence of a dependable methodology for early identification and limited therapeutic options for advanced disease. However, it takes over 17 years to develop pancreatic cancer from initiation of mutation to metastatic cancer; therefore, if diagnosed early; it may increase overall survival dramatically, thus, providing a window of opportunity for early detection. Recently, genomic expression analysis defined 4 subtypes of pancreatic cancer based on mutated genes. Hence, we need simple and standard, minimally invasive test that can monitor those altered genes or their associated pathways in time for the success of precision medicine, and liquid biopsy seems to be one answer to all these questions. Again, liquid biopsy has an ability to pair with genomic tests. Additionally, liquid biopsy based development of circulating tumor cells derived xenografts, 3D organoids system, real-time monitoring of genetic mutations by circulating tumor DNA and exosome as the targeted drug delivery vehicle holds lots of potential for the treatment and cure of pancreatic cancer. At present, diagnosis of pancreatic cancer is frantically done on the premise of CA19-9 and radiological features only, which doesn't give a picture of genetic mutations and epigenetic alteration involved. In this manner, the current diagnostic paradigm for pancreatic cancer diagnosis experiences low diagnostic accuracy. This review article discusses the current state of liquid biopsy in pancreatic cancer as diagnostic and therapeutic tools and future perspectives of research in the light of circulating tumor cells, circulating tumor DNA and exosomes.
Keywords: circulating tumor cells; circulating tumor nucleic acids; exosomes; liquid biopsy; pancreatic cancer.
Conflict of interest statement
CONFLICTS OF INTEREST Authors declare no competing interests.
Figures
Similar articles
-
Circulating tumor DNA as a liquid biopsy target for detection of pancreatic cancer.World J Gastroenterol. 2016 Oct 14;22(38):8480-8488. doi: 10.3748/wjg.v22.i38.8480. World J Gastroenterol. 2016. PMID: 27784960 Free PMC article. Review.
-
Circulating Liquid Biopsy Biomarkers in Glioblastoma: Advances and Challenges.Int J Mol Sci. 2024 Jul 21;25(14):7974. doi: 10.3390/ijms25147974. Int J Mol Sci. 2024. PMID: 39063215 Free PMC article. Review.
-
Liquid biopsy leads to a paradigm shift in the treatment of pancreatic cancer.World J Gastroenterol. 2022 Dec 14;28(46):6478-6496. doi: 10.3748/wjg.v28.i46.6478. World J Gastroenterol. 2022. PMID: 36569270 Free PMC article. Review.
-
Pancreatic Cancer Diagnosis and Management: Has the Time Come to Prick the Bubble?Front Endocrinol (Lausanne). 2019 Jan 8;9:779. doi: 10.3389/fendo.2018.00779. eCollection 2018. Front Endocrinol (Lausanne). 2019. PMID: 30671023 Free PMC article. Review.
-
The systematic role of pancreatic cancer exosomes: distant communication, liquid biopsy and future therapy.Cancer Cell Int. 2024 Jul 25;24(1):264. doi: 10.1186/s12935-024-03456-5. Cancer Cell Int. 2024. PMID: 39054529 Free PMC article. Review.
Cited by
-
A Novel Tissue-Free Method to Estimate Tumor-Derived Cell-Free DNA Quantity Using Tumor Methylation Patterns.Cancers (Basel). 2023 Dec 23;16(1):82. doi: 10.3390/cancers16010082. Cancers (Basel). 2023. PMID: 38201510 Free PMC article.
-
Usefulness of rapid on-site evaluation specimens from endoscopic ultrasound-guided fine-needle aspiration for cancer gene panel testing: A retrospective study.PLoS One. 2020 Jan 30;15(1):e0228565. doi: 10.1371/journal.pone.0228565. eCollection 2020. PLoS One. 2020. PMID: 31999789 Free PMC article.
-
Liquid Biopsy in Pancreatic Cancer: Are We Ready to Apply It in the Clinical Practice?Cancers (Basel). 2021 Apr 20;13(8):1986. doi: 10.3390/cancers13081986. Cancers (Basel). 2021. PMID: 33924143 Free PMC article. Review.
-
Circulating extracellular vesicle-encapsulated HULC is a potential biomarker for human pancreatic cancer.Cancer Sci. 2020 Jan;111(1):98-111. doi: 10.1111/cas.14232. Epub 2019 Dec 5. Cancer Sci. 2020. PMID: 31715081 Free PMC article.
-
Molecular pathology and protein markers for pancreatic cancer: relevance in staging, in adjuvant therapy, in determination of minimal residual disease, and follow-up.Hepatobiliary Surg Nutr. 2024 Feb 1;13(1):56-70. doi: 10.21037/hbsn-22-628. Epub 2023 Aug 14. Hepatobiliary Surg Nutr. 2024. PMID: 38322203 Free PMC article. Review.
References
-
- Court CM, Ankeny JS, Hou S, Tseng HR, Tomlinson JS. Improving pancreatic cancer diagnosis using circulating tumor cells: prospects for staging and single-cell analysis. Expert Rev Mol Diagn. 2015;15:1491–504. https://doi.org/10.1586/14737159.2015.1091311. - DOI - PMC - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67:7–30. https://doi.org/10.3322/caac.21387. - DOI - PubMed
-
- Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, Jemal A, Yu XQ, He J. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–32. https://doi.org/10.3322/caac.21338. - DOI - PubMed
-
- Assifi MM, Lu X, Eibl G, Reber HA, Li G, Hines OJ. Neoadjuvant therapy in pancreatic adenocarcinoma: a meta-analysis of phase II trials. Surgery. 2011;150:466–73. https://doi.org/10.1016/j.surg.2011.07.006. - DOI - PMC - PubMed
-
- Shrikhande SV, Kleeff J, Reiser C, Weitz J, Hinz U, Esposito I, Schmidt J, Friess H, Buchler MW. Pancreatic resection for M1 pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2007;14:118–27. https://doi.org/10.1245/s10434-006-9131-8. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
