

Nutritional status and muscle dysfunction in chronic respiratory diseases: stable phase versus acute exacerbations
- PMID: 29928517
- PMCID: PMC5989104
- DOI: 10.21037/jtd.2018.02.66
Nutritional status and muscle dysfunction in chronic respiratory diseases: stable phase versus acute exacerbations
Abstract
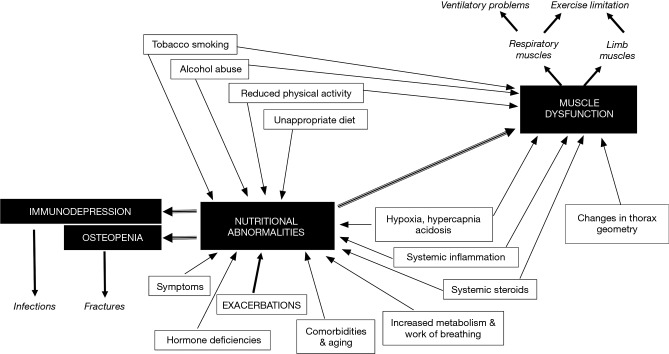
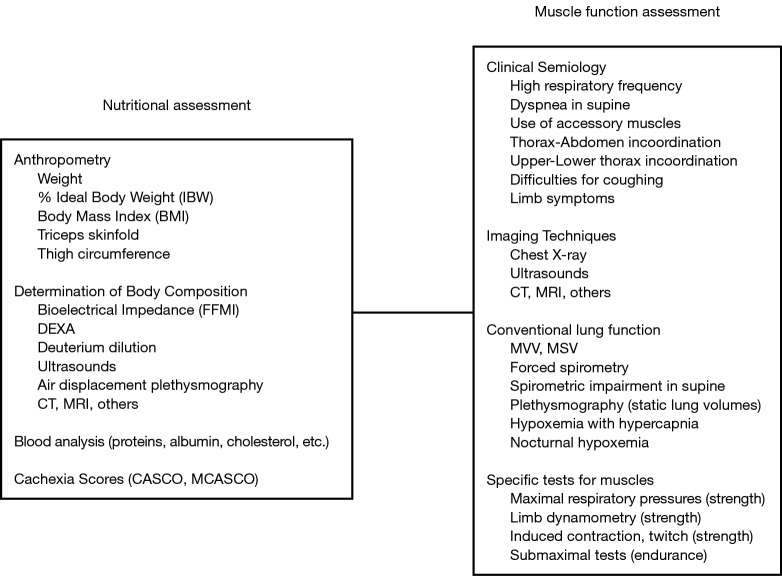
Nutritional abnormalities are frequent in different chronic respiratory diseases such as chronic obstructive pulmonary disease (COPD), bronchiectasis, cystic fibrosis (CF), interstitial fibrosis and lung cancer, having important clinical consequences. However, nutritional abnormalities often remained underdiagnosed due to the relative lack of awareness of health professionals. Therefore, systematic anthropometry or even better, assessment of body composition, should be performed in all patients with chronic respiratory conditions, especially following exacerbation periods when malnutrition becomes more accentuated. Nutritional abnormalities very often include the loss of muscle mass, which is an important factor for the occurrence of muscle dysfunction. The latter can be easily detected with the specific assessment of muscle strength and endurance, and also negatively influences patients' quality of life and prognosis. Both nutritional abnormalities and muscle dysfunction result from the interaction of several factors, including tobacco smoking, low physical activity-sedentarism, systemic inflammation and the imbalance between energy supply and requirements, which essentially lead to a negative balance between protein breakdown and synthesis. Therapeutic approaches include improvements in lifestyle, nutritional supplementation and training. Anabolic drugs may be administered in some cases.
Keywords: Nutritional abnormalities; diet; exercise; low body weight; lung diseases; muscle dysfunction; muscle mass; prognosis.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
[Chinese experts consensus statement: diagnosis and treatment of cystic fibrosis (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2023 Apr 12;46(4):352-372. doi: 10.3760/cma.j.cn112147-20221214-00971. Zhonghua Jie He He Hu Xi Za Zhi. 2023. PMID: 36990700 Chinese.
-
[Nutritional abnormalities in chronic obstructive pulmonary disease].Med Clin (Barc). 2014 Jul 22;143(2):78-84. doi: 10.1016/j.medcli.2013.05.040. Epub 2013 Sep 18. Med Clin (Barc). 2014. PMID: 24054776 Review. Spanish.
-
Clinical management of chronic obstructive pulmonary disease patients with muscle dysfunction.J Thorac Dis. 2016 Nov;8(11):3379-3400. doi: 10.21037/jtd.2016.11.105. J Thorac Dis. 2016. PMID: 28066619 Free PMC article. Review.
-
Can muscle protein metabolism be specifically targeted by nutritional support and exercise training in chronic obstructive pulmonary disease?J Thorac Dis. 2018 May;10(Suppl 12):S1377-S1389. doi: 10.21037/jtd.2018.05.81. J Thorac Dis. 2018. PMID: 29928520 Free PMC article. Review.
-
Computer Tomography (CT)-based Screening of Hospitalized Patients with Moderate to Severe Chronic Obstructive Pulmonary Disease Complicated by Bronchiectasis Phenotype During Acute Exacerbation: A Clinical Analysis.Curr Med Imaging. 2023 May 8. doi: 10.2174/1573405620666230508103841. Online ahead of print. Curr Med Imaging. 2023. PMID: 37157216
Cited by
-
Roles of Mesenchymal Cells in the Lung: From Lung Development to Chronic Obstructive Pulmonary Disease.Cells. 2021 Dec 9;10(12):3467. doi: 10.3390/cells10123467. Cells. 2021. PMID: 34943975 Free PMC article. Review.
-
Prognostic Value of Concomitant Bronchiectasis in Newly Diagnosed Diffuse Panbronchiolitis Patients on a Maintenance Therapy with Macrolides.Can Respir J. 2019 Mar 10;2019:4913814. doi: 10.1155/2019/4913814. eCollection 2019. Can Respir J. 2019. PMID: 30984318 Free PMC article.
-
Adaptive NKG2C+ natural killer cells are related to exacerbations and nutritional abnormalities in COPD patients.Respir Res. 2020 Mar 4;21(1):63. doi: 10.1186/s12931-020-1323-4. Respir Res. 2020. PMID: 32131843 Free PMC article.
-
Breathing and balance: Clinical insights and management strategies of respiratory acid-base disorders.Nutr Clin Pract. 2025 Aug;40(4):774-792. doi: 10.1002/ncp.11328. Epub 2025 Jun 8. Nutr Clin Pract. 2025. PMID: 40483586 Free PMC article. Review.
-
The Nutritional Status of Chronic Obstructive Pulmonary Disease Exacerbators.Can Respir J. 2022 Oct 13;2022:3101486. doi: 10.1155/2022/3101486. eCollection 2022. Can Respir J. 2022. PMID: 36276928 Free PMC article.
References
-
- Vogelmeier CF, Criner GJ, Martínez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report: GOLD Executive Summary. Arch Bronconeumol 2017;53:128-49. - PubMed
-
- Gea J, Barreiro E, Orozco-Levi M. Skeletal muscle adaptations to disease states. Chapter 11. In: Bottinelli R, Reggiani C. editors. Skeletal Muscle Plasticity in Health and Disease: From Genes to Whole Muscle. Dordrecht: Springer, 2006:315-60.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources