

Loss of Metabolic Flexibility in the Failing Heart
- PMID: 29928647
- PMCID: PMC5997788
- DOI: 10.3389/fcvm.2018.00068
Loss of Metabolic Flexibility in the Failing Heart
Abstract
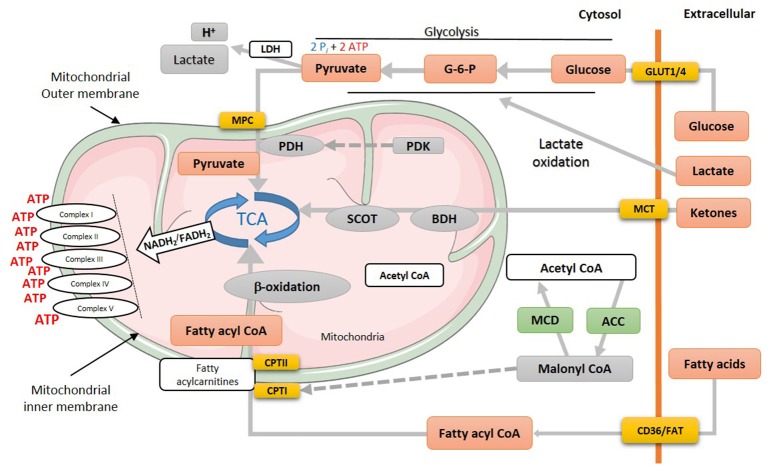
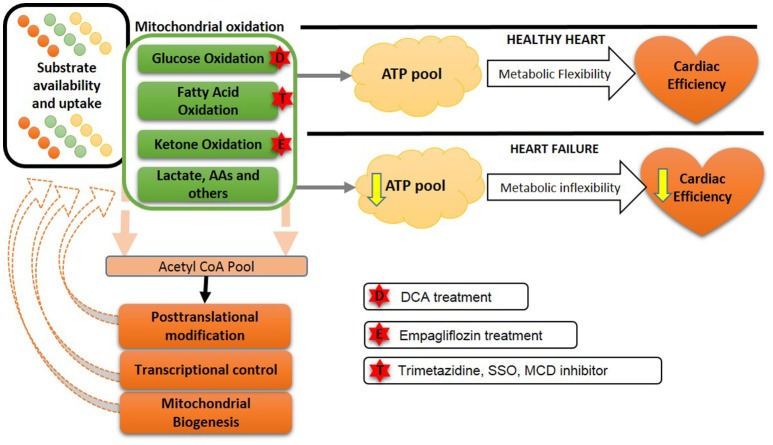
To maintain its high energy demand the heart is equipped with a highly complex and efficient enzymatic machinery that orchestrates ATP production using multiple energy substrates, namely fatty acids, carbohydrates (glucose and lactate), ketones and amino acids. The contribution of these individual substrates to ATP production can dramatically change, depending on such variables as substrate availability, hormonal status and energy demand. This "metabolic flexibility" is a remarkable virtue of the heart, which allows utilization of different energy substrates at different rates to maintain contractile function. In heart failure, cardiac function is reduced, which is accompanied by discernible energy metabolism perturbations and impaired metabolic flexibility. While it is generally agreed that overall mitochondrial ATP production is impaired in the failing heart, there is less consensus as to what actual switches in energy substrate preference occur. The failing heart shift toward a greater reliance on glycolysis and ketone body oxidation as a source of energy, with a decrease in the contribution of glucose oxidation to mitochondrial oxidative metabolism. The heart also becomes insulin resistant. However, there is less consensus as to what happens to fatty acid oxidation in heart failure. While it is generally believed that fatty acid oxidation decreases, a number of clinical and experimental studies suggest that fatty acid oxidation is either not changed or is increased in heart failure. Of importance, is that any metabolic shift that does occur has the potential to aggravate cardiac dysfunction and the progression of the heart failure. An increasing body of evidence shows that increasing cardiac ATP production and/or modulating cardiac energy substrate preference positively correlates with heart function and can lead to better outcomes. This includes increasing glucose and ketone oxidation and decreasing fatty acid oxidation. In this review we present the physiology of the energy metabolism pathways in the heart and the changes that occur in these pathways in heart failure. We also look at the interventions which are aimed at manipulating the myocardial metabolic pathways toward more efficient substrate utilization which will eventually improve cardiac performance.
Keywords: cardiac metabolism; fatty acid oxidation; glucose oxidation; heart failure; insulin resistant; ketone oxidation.
Figures

References
-
- Wang G, Zhang Z, Ayala C, Wall HK, Fang J. Costs of heart failure-related hospitalizations in patients aged 18 to 64 years. Am J Manag Care (2010) 16:769–76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical