

Modelling the impact of antimalarial quality on the transmission of sulfadoxine-pyrimethamine resistance in Plasmodium falciparum
- PMID: 29928735
- PMCID: PMC6001968
- DOI: 10.1016/j.idm.2017.04.001
Modelling the impact of antimalarial quality on the transmission of sulfadoxine-pyrimethamine resistance in Plasmodium falciparum
Abstract
Background: The use of poor quality antimalarial medicines, including the use of non-recommended medicines for treatment such as sulfadoxine-pyrimethamine (SP) monotherapy, undermines malaria control and elimination efforts. Furthermore, the use of subtherapeutic doses of the active ingredient(s) can theoretically promote the emergence and transmission of drug resistant parasites.
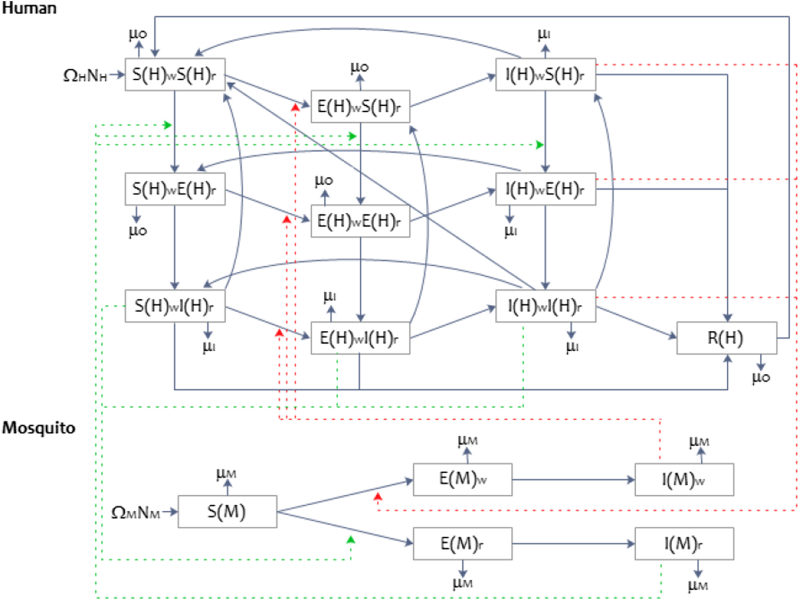
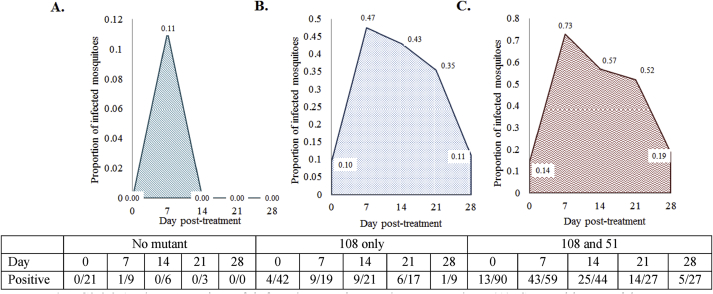
Methods: We developed a deterministic compartmental model to quantify the impact of antimalarial medicine quality on the transmission of SP resistance, and validated it using sensitivity analysis and a comparison with data from Kenya collected in 2006. We modelled human and mosquito population dynamics, incorporating two Plasmodium falciparum subtypes (SP-sensitive and SP-resistant) and both poor quality and good quality (artemether-lumefantrine) antimalarial use.
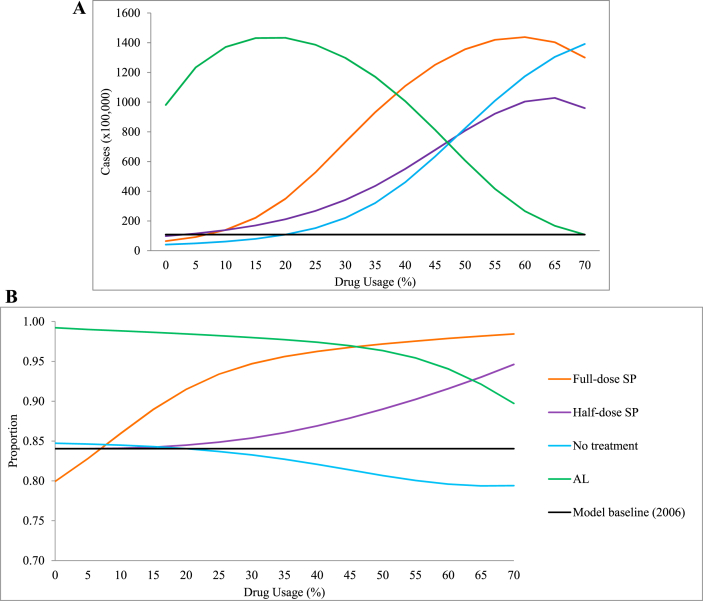
Findings: The model predicted that an increase in human malaria cases, and among these, an increase in the proportion of SP-resistant infections, resulted from an increase in poor quality SP antimalarial use, whether it was full- or half-dose SP monotherapy.
Interpretation: Our findings suggest that an increase in poor quality antimalarial use predicts an increase in the transmission of resistance. This highlights the need for stricter control and regulation on the availability and use of poor quality antimalarial medicines, in order to offer safe and effective treatments, and work towards the eradication of malaria.
Keywords: Antimalarial quality; Deterministic compartmental model; Drug resistance; Falsified antimalarial medicine; Plasmodium falciparum malaria; Substandard antimalarial treatments.
Figures
References
-
- Anderson R.M., May R.M. Oxford University Press; 1991. Infectious diseases of humans: Dynamics and control.
-
- Barnes K.I., White N.J. Population biology and antimalarial resistance: The transmission of antimalarial drug resistance in Plasmodium falciparum. Acta Tropica. 2005;94:230–240. - PubMed
-
- Barnes K.I., Little F., Mabuza A., Mngomezulu N., Govere J., Durrheim D.…White N.J. Increased gametocytemia after treatment: An early parasitological indicator of emerging Sulfadoxine-Pyrimethamine resistance in falciparum malaria. The Journal of Infectious Diseases. 2008;197:1605–1613. - PubMed
-
- Barnes K., Watkins W., White N. Antimalarial dosing regimens and drug resistance. Trends in Parasitology. 2008;24(3):127–134. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
