Glutamatergic Deficits in Schizophrenia - Biomarkers and Pharmacological Interventions within the Ketamine Model
- PMID: 29929462
- PMCID: PMC6142413
- DOI: 10.2174/1389201019666180620112528
Glutamatergic Deficits in Schizophrenia - Biomarkers and Pharmacological Interventions within the Ketamine Model
Abstract
Background: The observation that N-methyl-D-aspartate glutamate receptor (NMDAR) antagonists such as ketamine transiently induce schizophrenia-like positive, negative and cognitive symptoms has led to a paradigm shift from dopaminergic to glutamatergic dysfunction in pharmacological models of schizophrenia. NMDAR hypofunction can explain many schizophrenia symptoms directly due to excitatory-to-inhibitory (E/I) imbalance, but also dopaminergic dysfunction itself. However, so far no new drug targeting the NMDAR has been successfully approved. In the search for possible biomarkers it is interesting that ketamine-induced psychopathological changes in healthy participants were accompanied by altered electro-(EEG), magnetoencephalographic (MEG) and functional magnetic resonance imaging (fMRI) signals.
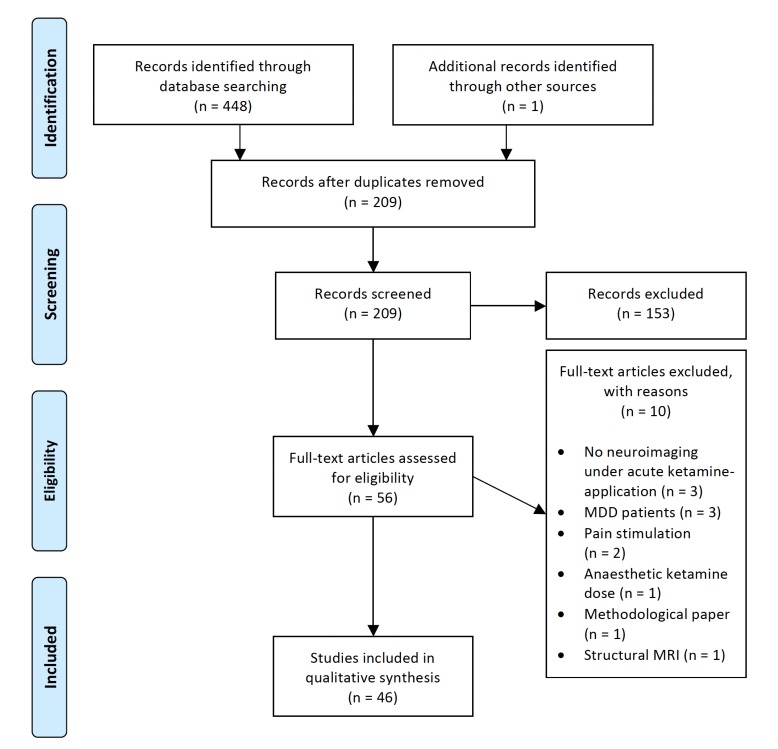
Methods: We systematically searched PubMed/Medline and Web of Knowledge databases (January 2006 to July 2017) to identify EEG/MEG and fMRI studies of the ketamine model of schizophrenia with human subjects. The search strategy identified 209 citations of which 46 articles met specified eligibility criteria.
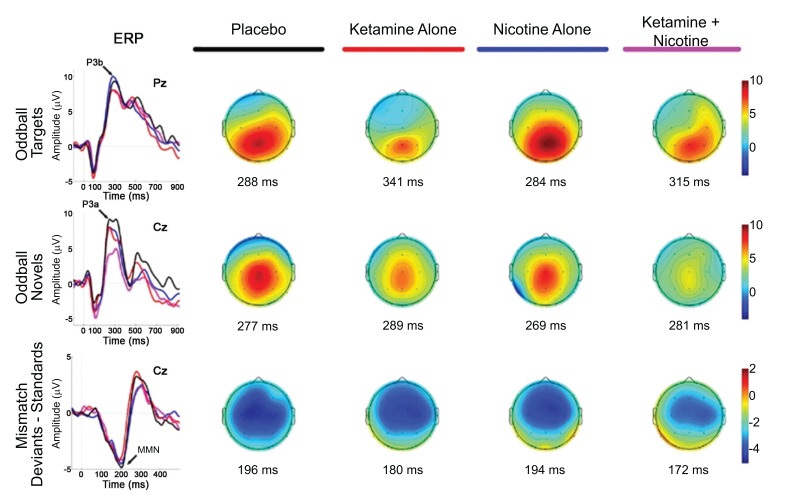
Results: In EEG/MEG studies, ketamine induced changes of event-related potentials, such as the P300 potential and the mismatch negativity, similar to alterations observed in schizophrenia patients. In fMRI studies, alterations of activation were observed in different brain regions, most prominently within the anterior cingulate cortex and limbic structures as well as task-relevant brain regions. These alterations were accompanied by changes in functional connectivity, indicating a balance shift of the underlying brain networks. Pharmacological treatments did alter ketamine-induced changes in EEG/MEG and fMRI studies to different extents.
Conclusion: This review highlights the potential applicability of the ketamine model for schizophrenia drug development by offering the possibility to assess the effect of pharmacological agents on schizophrenia- like symptoms and to find relevant neurophysiological and neuroimaging biomarkers.
Keywords: EEG; MEG; NMDA-receptor; fMRI; ketamine; schizophrenia..
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.org.
Figures
Similar articles
-
Glutamatergic deficit and schizophrenia-like negative symptoms: new evidence from ketamine-induced mismatch negativity alterations in healthy male humans.J Psychiatry Neurosci. 2017 Jun;42(4):273-283. doi: 10.1503/jpn.160187. J Psychiatry Neurosci. 2017. PMID: 28556775 Free PMC article. Clinical Trial.
-
NMDA hypofunction in the posterior cingulate as a model for schizophrenia: an exploratory ketamine administration study in fMRI.Schizophr Res. 2005 Jan 1;72(2-3):235-48. doi: 10.1016/j.schres.2004.04.009. Schizophr Res. 2005. PMID: 15560968 Clinical Trial.
-
Glutamate and schizophrenia: phencyclidine, N-methyl-D-aspartate receptors, and dopamine-glutamate interactions.Int Rev Neurobiol. 2007;78:69-108. doi: 10.1016/S0074-7742(06)78003-5. Int Rev Neurobiol. 2007. PMID: 17349858 Review.
-
Ketamine effects on brain function--simultaneous fMRI/EEG during a visual oddball task.Neuroimage. 2011 Sep 15;58(2):508-25. doi: 10.1016/j.neuroimage.2011.06.045. Epub 2011 Jun 29. Neuroimage. 2011. PMID: 21723949 Clinical Trial.
-
Has an angel shown the way? Etiological and therapeutic implications of the PCP/NMDA model of schizophrenia.Schizophr Bull. 2012 Sep;38(5):958-66. doi: 10.1093/schbul/sbs069. Schizophr Bull. 2012. PMID: 22987851 Free PMC article. Review.
Cited by
-
Dysfunction of the NMDA Receptor in the Pathophysiology of Schizophrenia and/or the Pathomechanisms of Treatment-Resistant Schizophrenia.Biomolecules. 2024 Sep 6;14(9):1128. doi: 10.3390/biom14091128. Biomolecules. 2024. PMID: 39334894 Free PMC article. Review.
-
Dopamine, Psychosis, and Symptom Fluctuation: A Narrative Review.Healthcare (Basel). 2022 Sep 7;10(9):1713. doi: 10.3390/healthcare10091713. Healthcare (Basel). 2022. PMID: 36141325 Free PMC article. Review.
-
Neurobehavioral Differences of Valproate and Risperidone on MK-801 Inducing Acute Hyperlocomotion in Mice.Behav Neurol. 2022 Feb 23;2022:1048463. doi: 10.1155/2022/1048463. eCollection 2022. Behav Neurol. 2022. PMID: 35251367 Free PMC article.
-
Ketamine Alters Functional Gamma and Theta Resting-State Connectivity in Healthy Humans: Implications for Schizophrenia Treatment Targeting the Glutamate System.Front Psychiatry. 2021 Jun 10;12:671007. doi: 10.3389/fpsyt.2021.671007. eCollection 2021. Front Psychiatry. 2021. PMID: 34177660 Free PMC article.
-
A multicenter study of ketamine effects on functional connectivity: Large scale network relationships, hubs and symptom mechanisms.Neuroimage Clin. 2019;22:101739. doi: 10.1016/j.nicl.2019.101739. Epub 2019 Feb 28. Neuroimage Clin. 2019. PMID: 30852397 Free PMC article.
References
-
- Miyamoto S., Miyake N., Jarskog L.F., Fleischhacker W.W., Lieberman J.A. Pharmacological treatment of schizophrenia: A critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol. Psychiatry. 2012;17(12):1206–1227. - PubMed
-
- Poels E.M., Kegeles L.S., Kantrowitz J.T., Slifstein M., Javitt D.C., Lieberman J.A., Abi-Dargham A., Girgis R.R. Imaging glutamate in schizophrenia: Review of findings and implications for drug discovery. Mol. Psychiatry. 2014;19(1):20–29. - PubMed
-
- Miyamoto S., Duncan G.E., Marx C.E., Lieberman J.A. Treatments for schizophrenia: A critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol. Psychiatry. 2005;10(1):79–104. - PubMed
-
- Luby E.D., Gottlieb J.S., Cohen B.D., Rosenbaum G., Domino E.F. Model psychoses and schizophrenia. Am. J. Psychiatry. 1962;119:61–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous