

Contemporary rates and predictors of fast progression of chronic kidney disease in adults with and without diabetes mellitus
- PMID: 29929484
- PMCID: PMC6014002
- DOI: 10.1186/s12882-018-0942-1
Contemporary rates and predictors of fast progression of chronic kidney disease in adults with and without diabetes mellitus
Abstract
Background: Chronic kidney disease (CKD) is highly prevalent but identification of patients at high risk for fast CKD progression before reaching end-stage renal disease in the short-term has been challenging. Whether factors associated with fast progression vary by diabetes status is also not well understood. We examined a large community-based cohort of adults with CKD to identify predictors of fast progression during the first 2 years of follow-up in the presence or absence of diabetes mellitus.
Methods: Within a large integrated healthcare delivery system in northern California, we identified adults with estimated glomerular filtration rate (eGFR) 30-59 ml/min/1.73 m2 by CKD-EPI equation between 2008 and 2010 who had no previous dialysis or renal transplant, who had outpatient serum creatinine values spaced 10-14 months apart and who did not initiate renal replacement therapy, die or disenroll during the first 2 years of follow-up. Through 2012, we calculated the annual rate of change in eGFR and classified patients as fast progressors if they lost > 4 ml/min/1.73 m2 per year. We used multivariable logistic regression to identify patient characteristics that were independently associated with fast CKD progression stratified by diabetes status.
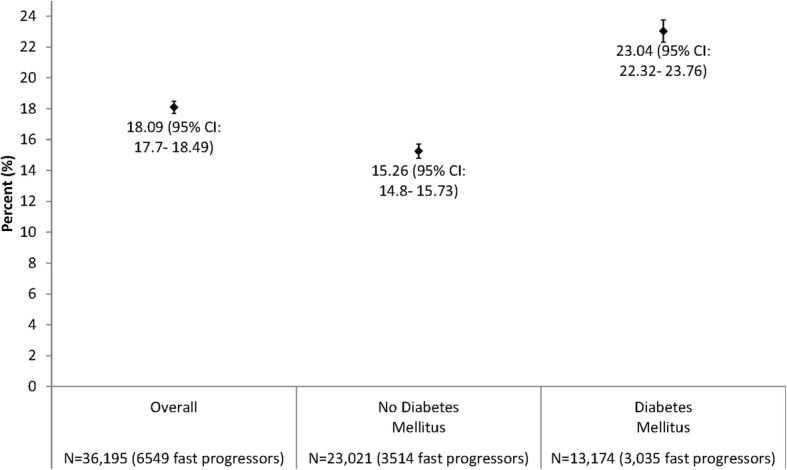
Results: We identified 36,195 eligible adults with eGFR 30-59 ml/min/1.73 m2 and mean age 73 years, 55% women, 11% black, 12% Asian/Pacific Islander and 36% with diabetes mellitus. During 24-month follow-up, fast progression of CKD occurred in 23.0% of patients with diabetes vs. 15.3% of patients without diabetes. Multivariable predictors of fast CKD progression that were similar by diabetes status included proteinuria, age ≥ 80 years, heart failure, anemia and higher systolic blood pressure. Age 70-79 years, prior ischemic stroke, current or former smoking and lower HDL cholesterol level were also predictive in patients without diabetes, while age 18-49 years was additionally predictive in those with diabetes.
Conclusions: In a large, contemporary population of adults with eGFR 30-59 ml/min/1.73 m2, accelerated progression of kidney dysfunction within 2 years affected ~ 1 in 4 patients with diabetes and ~ 1 in 7 without diabetes. Regardless of diabetes status, the strongest independent predictors of fast CKD progression included proteinuria, elevated systolic blood pressure, heart failure and anemia.
Keywords: Anemia; Blood pressure; Chronic kidney disease; Diabetes; Progression; Proteinuria; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Kaiser Permanente Northern California institutional review board. A waiver of consent was obtained due to the nature of the study.
Consent for publication
Not applicable.
Competing interests
Drs. Cabrera, Stefansson and Greasley are employees of Astra-Zeneca. Ms. Yang, Ms. Tan and Dr. Ordonez declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
