

SOCIETY FOR ENDOCRINOLOGY CLINICAL GUIDANCE: Inpatient management of cranial diabetes insipidus
- PMID: 29930026
- PMCID: PMC6013691
- DOI: 10.1530/EC-18-0154
SOCIETY FOR ENDOCRINOLOGY CLINICAL GUIDANCE: Inpatient management of cranial diabetes insipidus
Abstract
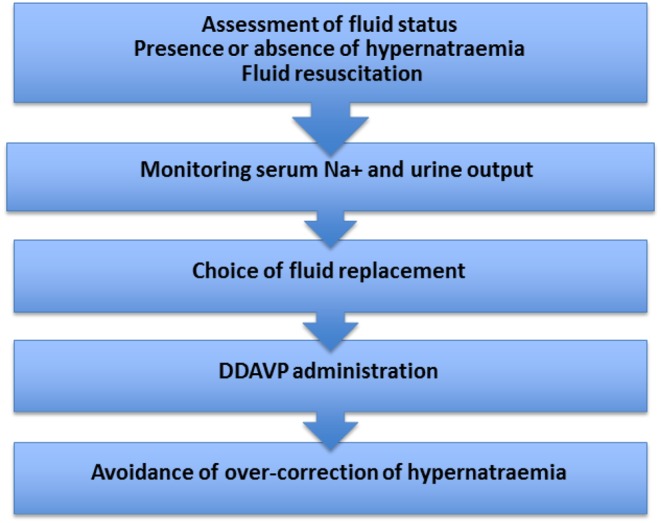
Cranial diabetes insipidus (CDI) is a treatable chronic condition that can potentially develop into a life-threatening medical emergency. CDI is due to the relative or absolute lack of the posterior pituitary hormone vasopressin (AVP), also known as anti-diuretic hormone. AVP deficiency results in uncontrolled diuresis. Complete deficiency can lead to polyuria exceeding 10 L/24 h. Given a functioning thirst mechanism and free access to water, patients with CDI can normally maintain adequate fluid balance through increased drinking. Desmopressin (DDAVP, a synthetic AVP analogue) reduces uncontrolled water excretion in CDI and is commonly used in treatment. Critically, loss of thirst perception (through primary pathology or reduced consciousness) or limited access to water (through non-availability, disability or inter-current illness) in a patient with CDI can lead to life-threatening dehydration. This position can be further exacerbated through the omission of DDAVP. Recent data have highlighted serious adverse events (including deaths) in patients with CDI. These adverse outcomes and deaths have occurred through a combination of lack of knowledge and treatment failures by health professionals. Here, with our guideline, we recommend treatment pathways for patients with known CDI admitted to hospital. Following these guidelines is essential for the safe management of patients with CDI.
Keywords: DDAVP; desmopressin; diabetes insipidus; guideline; hypernatraemia; pituitary.
© 2018 Society for Endocrinology.
Figures
References
-
- NHS England Patient Safety Alert. Risk of severe harm or death when desmopressin is omitted or delayed in patients with cranial diabetes insipidus. Alert reference number: NHS/PSA/W/2016/001. Redditch, UK: NHS England, 2016. (available at: https://www.england.nhs.uk/2016/02/psa-desmopressin/)
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
