

Neuroimmunology of Behavioral Comorbidities Associated With Cancer and Cancer Treatments
- PMID: 29930550
- PMCID: PMC6001368
- DOI: 10.3389/fimmu.2018.01195
Neuroimmunology of Behavioral Comorbidities Associated With Cancer and Cancer Treatments
Abstract
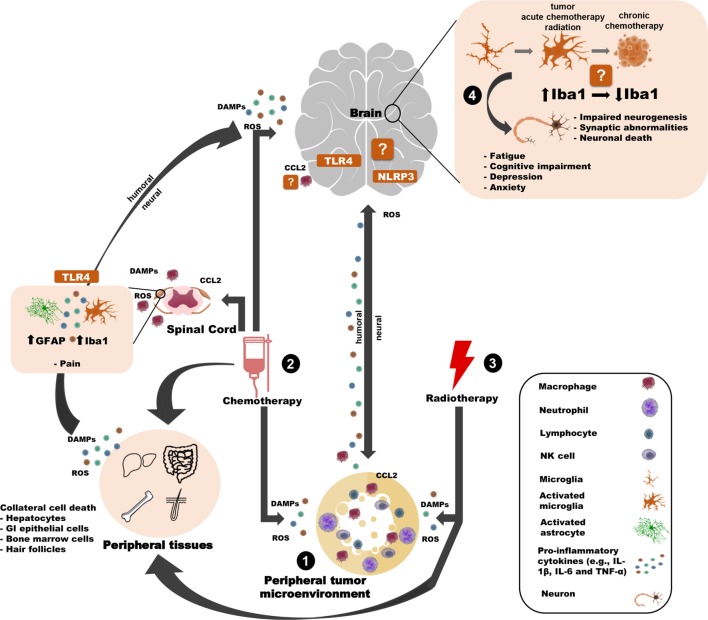
Behavioral comorbidities (depression, anxiety, fatigue, cognitive disturbances, and neuropathic pain) are prevalent in cancer patients and survivors. These mental and neurological health issues reduce quality-of-life, which is a significant societal concern given the increasing rates of long-term survival after various cancers. Hypothesized causes of behavioral comorbidities with cancer include tumor biology, stress associated with the cancer experience, and cancer treatments. A relatively recent leading mechanism by which these causes contribute to changes in neurobiology that underlie behavior is inflammation. Indeed, both basic and clinical research indicates that peripheral inflammation leads to central inflammation and behavioral changes in other illness contexts. Given the limitations of assessing neuroimmunology in clinical populations, this review primarily synthesizes evidence of neuroimmune and neuroinflammatory changes due to two components of cancer (tumor biology and cancer treatments) that are associated with altered affective-like or cognitive behaviors in rodents. Specifically, alterations in microglia, neuroinflammation, and immune trafficking to the brain are compiled in models of tumors, chemotherapy, and/or radiation. Evidence-based neuronal mechanisms by which these neuroimmune changes may lead to changes in behavior are proposed. Finally, converging evidence in clinical cancer populations is discussed.
Keywords: cognition; cytokines; depression; neuroinflammation; neuropathic pain.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical