

Tumor de corpo carotídeo (paraganglioma): relato de dois casos submetidos a tratamento cirúrgico
- PMID: 29930583
- PMCID: PMC5829712
- DOI: 10.1590/1677-5449.007315
Tumor de corpo carotídeo (paraganglioma): relato de dois casos submetidos a tratamento cirúrgico
Abstract
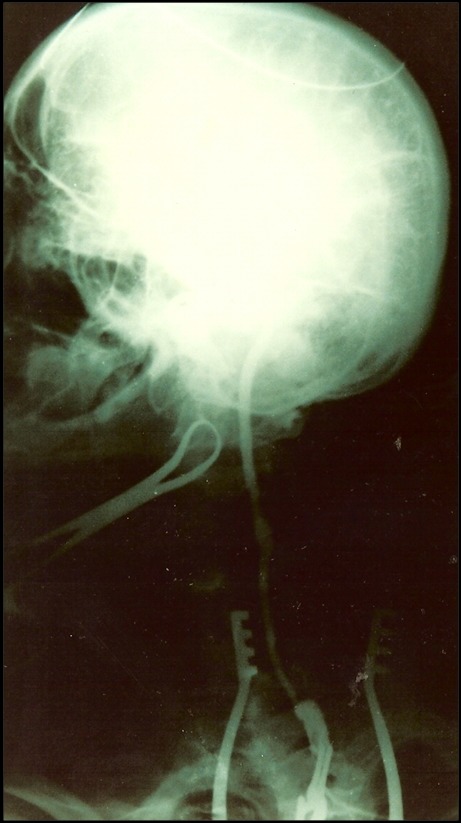
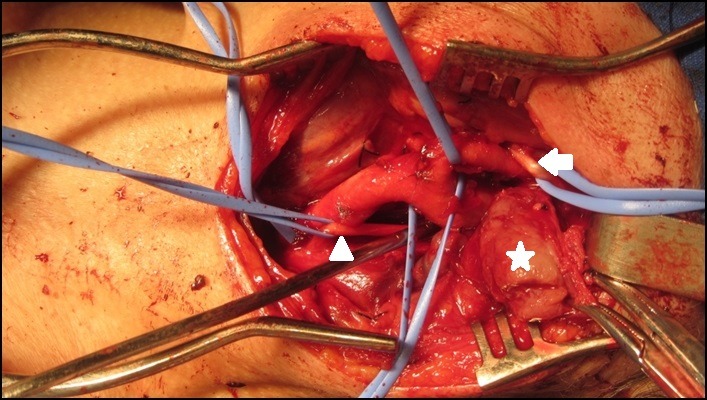
Abstract: A carotid body tumor is a rare neoplasm, generally benign, that predominantly affects people between their fourth and fifth decades of life. It manifests as a pulsatile and generally painless cervical mass with firm consistency, located below the angle of the jaw. It can progress to the extent that it causes localized pain, dysphagia, hiccups, hoarseness and hypersensitive carotid body syndrome. This article reports the cases of two female patients diagnosed with this tumor who were treated surgically. The first was treated with block resection of the tumor, while the second patient, who had an early stage tumor, was treated with subadventitial resection of the lesion.
O tumor de corpo carotídeo é uma neoplasia rara, geralmente benigna, que acomete, sobretudo, indivíduos entre a quarta e a quinta décadas de vida. Manifesta-se pela presença de massa cervical consistente localizada abaixo do ângulo da mandíbula, pulsátil e comumente indolor. Pode evoluir para dor local, disfagia, soluços, rouquidão e síndrome do corpo carotídeo hipersensível. Este artigo relata os casos de duas pacientes diagnosticadas com essa neoplasia e submetidas ao tratamento cirúrgico. A primeira foi submetida a uma ressecção em bloco do tumor, enquanto a segunda, com estadiamento mais precoce, foi tratada com uma ressecção subadventicial da lesão.
Conflict of interest statement
Conflito de interesse: Os autores declararam não haver conflitos de interesse que precisam ser informados.
Figures
















References
-
- Gaylis H, Davidge-Pitts K, Pantanowitz D. Carotid body tumors: a review of 52 cases. S Afr Med J. 1987;72(7):493–496. - PubMed
-
- Meyer FB, Sundt TM, Jr, Pearson BW. Carotid body tumors: a subject review and suggested surgical approach. J Neurosurg. 1986;64(3):377–385. http://dx.doi.org/10.3171/jns.1986.64.3.0377 - DOI - PubMed
-
- Shamblin WR, Remine WH, Sheps SG, Harrison EG. Carotid body tumor (chemodectoma). Clinicopathologic analysis of ninety cases. Am J Surg. 1971;122(6):732–739. http://dx.doi.org/10.1016/0002-9610(71)90436-3 - DOI - PubMed
-
- Patiño FT, Acosta FG, Guzman CP, Parada JM, Almedaro SL. Tumor de cuerpo carotídeo: análisis de 96 casos. Ver Invest Clin. 1991;43:119–123. - PubMed
-
- Davidovic LB, Djukic VB, Vasic DM, Sindjelic RP, Duvnjak SN. Diagnosis and treatment of carotid body paraganglioma: 21 years of experience at a clinical center of Serbia. World J Surg Oncol. 2005;3(1):10. http://dx.doi.org/10.1186/1477-7819-3-10 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources