

Extranodal Diffuse Large B Cell Lymphoma: Molecular Features, Prognosis, and Risk of Central Nervous System Recurrence
- PMID: 29931605
- PMCID: PMC6294323
- DOI: 10.1007/s11864-018-0555-8
Extranodal Diffuse Large B Cell Lymphoma: Molecular Features, Prognosis, and Risk of Central Nervous System Recurrence
Abstract
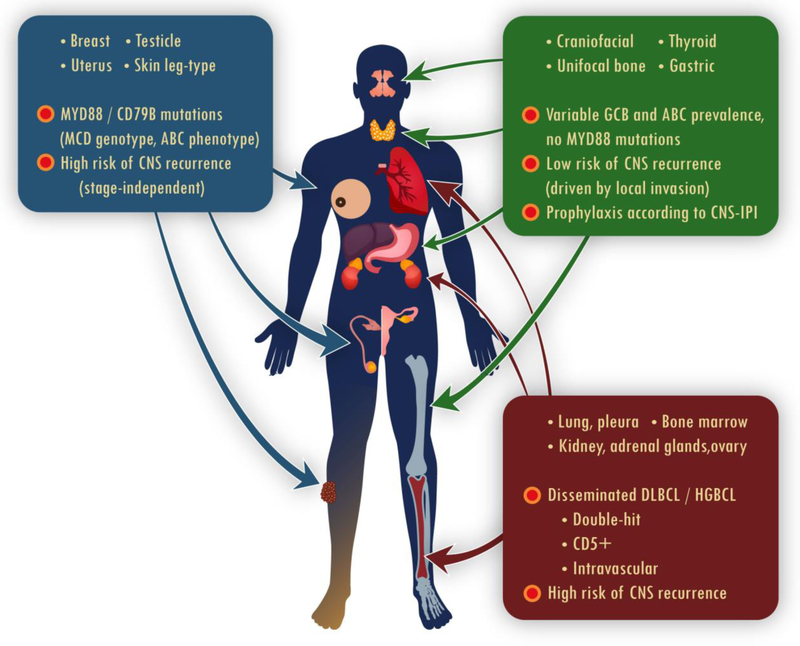
Diffuse large B cell lymphoma (DLBCL) arises from extranodal organs in about 30% of cases. Its prognosis and risk of recurrence in the central nervous system (CNS) vary according to the primary site of origin. Recent studies begin to clarify these differences using molecular classification. Testicular, breast, and uterine DLBCL (as well as possibly primary cutaneous DLBCL, leg-type) share a high prevalence of the non-germinal center B cell (non-GCB) phenotype and the MYD88/CD79B-mutated (MCD) genotype. These biologic features, which resemble primary CNS lymphoma, may underlie their stage-independent propensity for CNS involvement. Management of these lymphomas should involve CNS prophylaxis, preferably using systemic high-dose methotrexate to prevent intraparenchymal recurrence. Involvement of the kidneys, adrenal glands, ovary, bone marrow, lung, or pleura usually indicates disseminated disease, conferring worse prognosis. Involvement of these sites is often associated with high CNS-International Prognostic Index (IPI), concurrent MYC and BCL2 or BCL6 rearrangements, or intravascular lymphoma-risk factors warranting CNS prophylaxis. In contrast, craniofacial, thyroid, localized bone, or gastric lymphomas have a variable prevalence of the non-GCB phenotype and lack MYD88 mutations. Their outcomes with standard immunochemotherapy are excellent, and the risk of CNS recurrence is low. We recommend individualized consideration of CNS prophylaxis based on the CNS-IPI score and anatomical proximity in cases of epidural, orbital, or skull involvement. Rituximab-containing immunochemotherapy is a standard approach for all extranodal DLBCLs. Surgery is no longer required for any primary site, but routine consolidative radiation therapy is recommended for testicular lymphoma. Radiation therapy also appears to be associated with better progression-free survival in primary bone DLBCL. Future studies should better distinguish primary from secondary sites of extranodal involvement, and investigate the association of newly identified genotypes with the risk of CNS or systemic recurrence.
Keywords: Cell of origin; Central nervous system prophylaxis; Diffuse large B cell lymphoma; Extranodal lymphoma; MYD88; Radiation therapy.
Conflict of interest statement
Conflict of Interest
Thomas A. Ollila and Adam J. Olszewski declare they have no conflict of interest.
Figures
References
-
- Swerdlow SH, World Health Organization, International Agency for Research on Cancer WHO classification of tumours of haematopoietic and lymphoid tissues. Revised 4th edition ed. World Health Organization classification of tumours. Lyon: International Agency for Research on Cancer; 2017.
-
- Castillo JJ, Winer ES, Olszewski AJ. Sites of extranodal involvement are prognostic in patients with diffuse large B-cell lymphoma in the rituximab era: an analysis of the Surveillance, Epidemiology and End Results database. Am J Hematol 2014;89(3):310–4. doi:10.1002/ajh.23638. - DOI - PubMed
-
- El-Galaly TC, Villa D, Alzahrani M, Hansen JW, Sehn LH, Wilson D et al. Outcome prediction by extranodal involvement, IPI, R-IPI, and NCCN-IPI in the PET/CT and rituximab era: A Danish-Canadian study of 443 patients with diffuse-large B-cell lymphoma. Am J Hematol. 2015;90(11):1041–6. doi:10.1002/ajh.24169. - DOI - PubMed
-
- Hui D, Proctor B, Donaldson J, Shenkier T, Hoskins P, Klasa R et al. Prognostic implications of extranodal involvement in patients with diffuse large B-cell lymphoma treated with rituximab and cyclophosphamide, doxorubicin, vincristine, and prednisone. Leuk Lymphoma. 2010;51(9):1658–67. doi:10.3109/10428194.2010.504872. - DOI - PubMed
-
- Feugier P, Van Hoof A, Sebban C, Solal-Celigny P, Bouabdallah R, Ferme C et al. Long-term results of the R-CHOP study in the treatment of elderly patients with diffuse large B-cell lymphoma: a study by the Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol. 2005;23(18):4117–26. doi:10.1200/JCO.2005.09.131. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
