

External validation of a time-lapse model; a retrospective study comparing embryo evaluation using a morphokinetic model to standard morphology with live birth as endpoint
- PMID: 29932617
- PMCID: PMC6106632
- DOI: 10.5935/1518-0557.20180041
External validation of a time-lapse model; a retrospective study comparing embryo evaluation using a morphokinetic model to standard morphology with live birth as endpoint
Abstract
Objective: To validate a morphokinetic implantation model developed for EmbryoScope on embryos with known outcome, compared to standard morphology in a retrospective single center study.
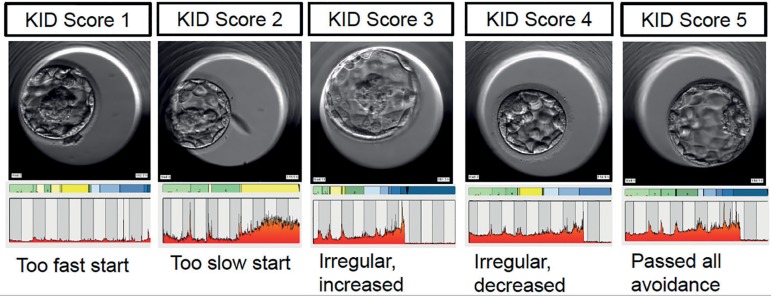
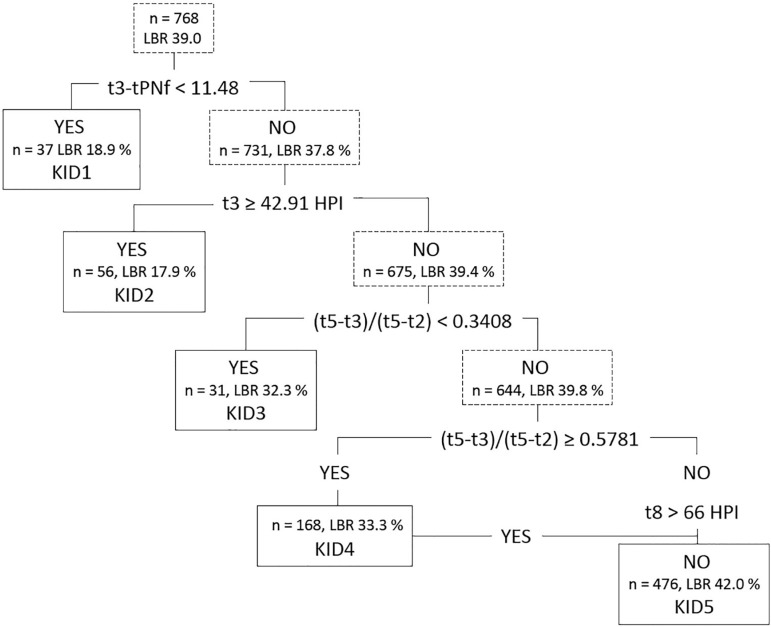
Methods: Morphokinetic annotation of 768 embryos with known outcome between 2013 -2015; corresponding to 116 D3 fresh embryos, 80 D6 frozen blastocysts, and 572 D5 blastocysts, fresh or frozen. The embryos were ranked by the KIDScore into five classes, KID1-5, and grouped into four classes based on standard morphology. Pregnancy rates, clinical pregnancy rates and live birth rates were compared. Combinations of morphology and morphokinetics were evaluated for implantation rates and live births.
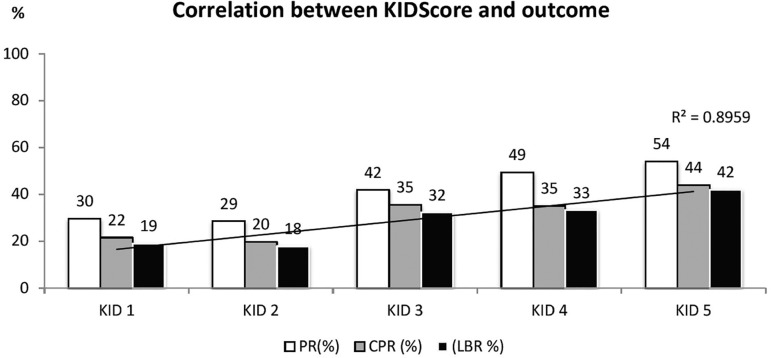
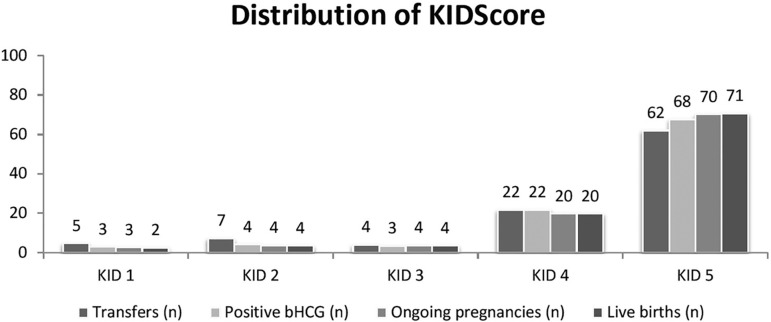
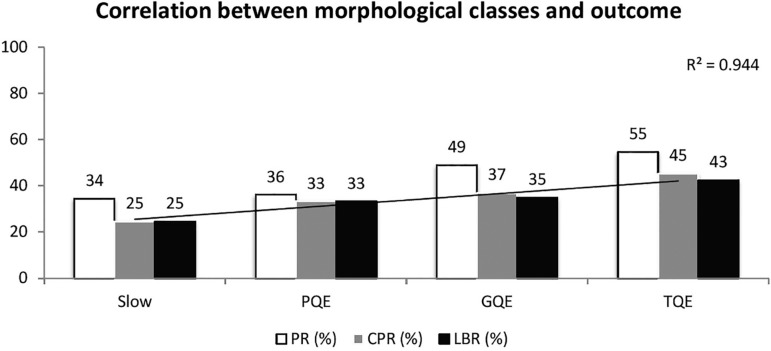
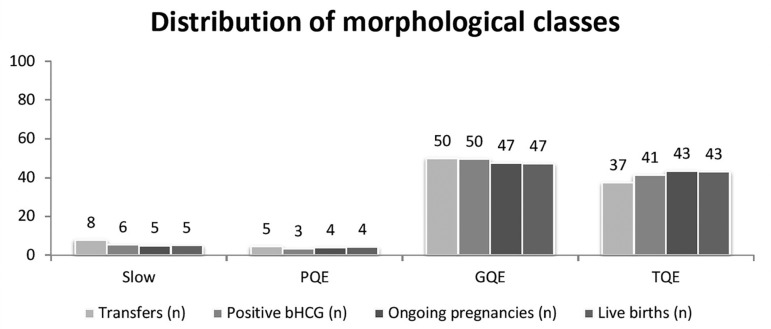
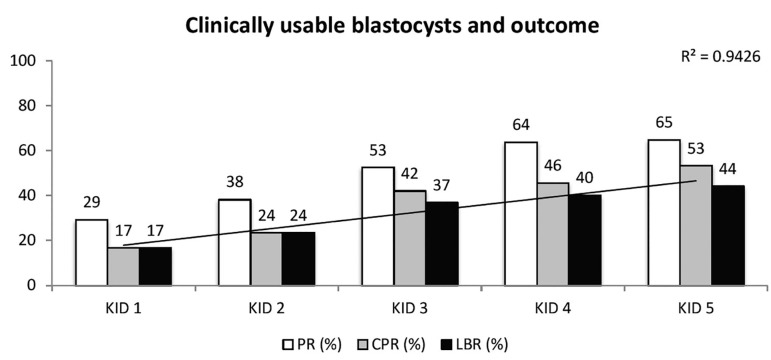
Results: Live birth rate increased with increasing KIDScore, from 19% for KID1 to 42% for KID5. Of all live births, KID5 contributed with 71%, KID4 with 20%, KID3 with 4%, KID2 with 4%, and KID1 with 2%. For morphology, the corresponding figure was 43% for Top Quality, 47% for Good Quality, 4% for Poor Quality, and 5% for Slow embryos. For day 3 embryos, KID5 embryos had the highest live birth rates, and contributed to 83% of the live births; whereas the second best morphological class had the highest live birth rate and contributed to most of the live births. For blastocysts, the KIDScore and morphology performed equally well. Combining morphology and morphokinetics indicated stronger predictive power for morphokinetics.
Conclusions: Overall, the KIDScore correlates with both implantation and live birth in our clinical setting. Compared to morphology, the KIDScore was superior for day 3 embryos, and equally good for blastocysts at predicting live births.
Keywords: Algorithm; embryo evaluation; embryo selection; morphokinetics; time-lapse image.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources