

Integration of resting state functional MRI into clinical practice - A large single institution experience
- PMID: 29933375
- PMCID: PMC6014724
- DOI: 10.1371/journal.pone.0198349
Integration of resting state functional MRI into clinical practice - A large single institution experience
Abstract
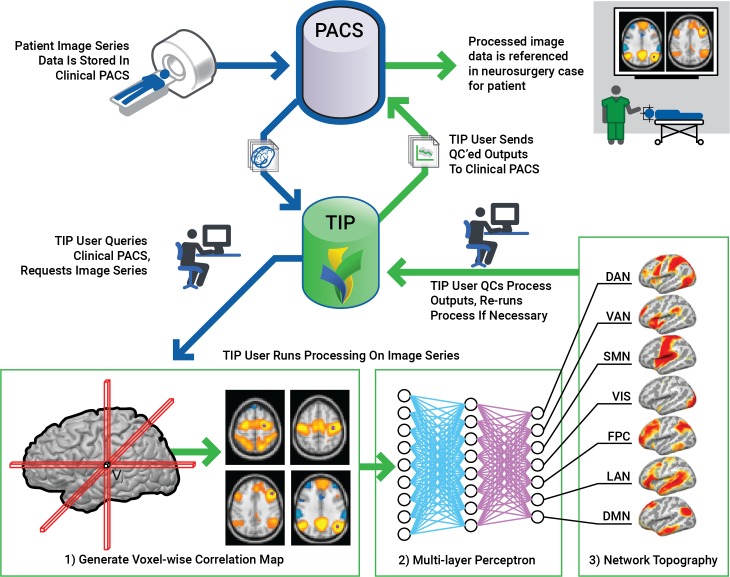
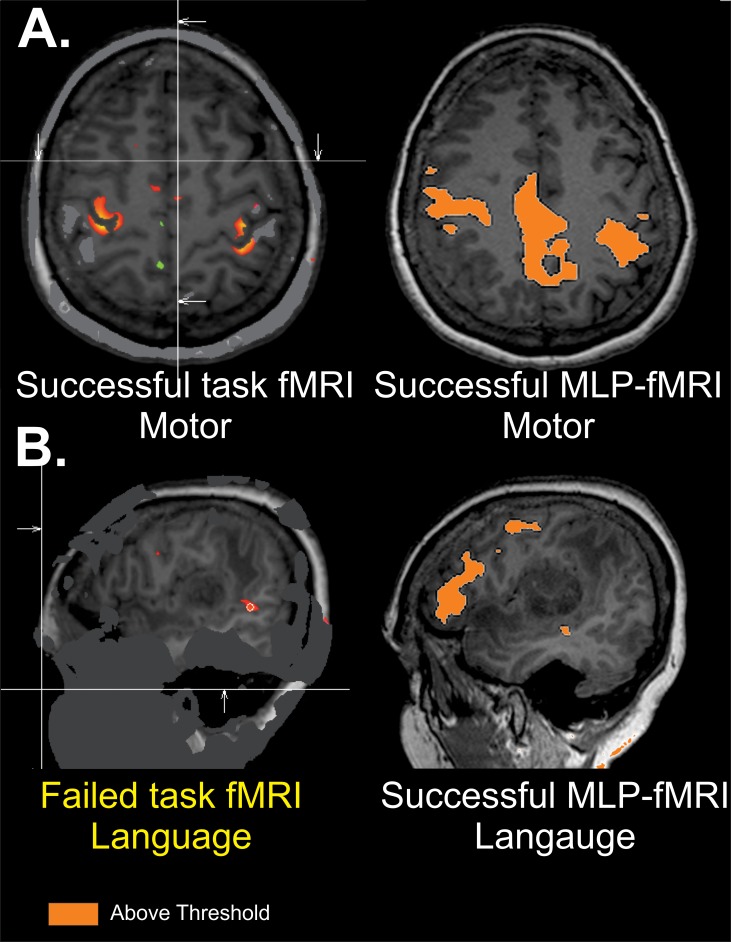
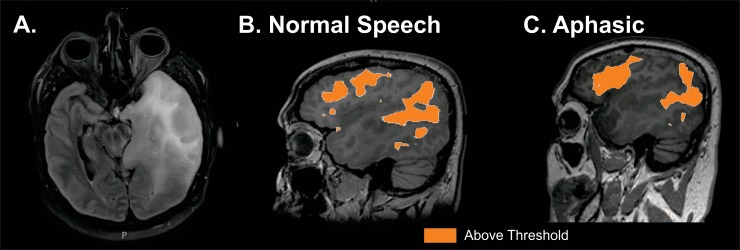
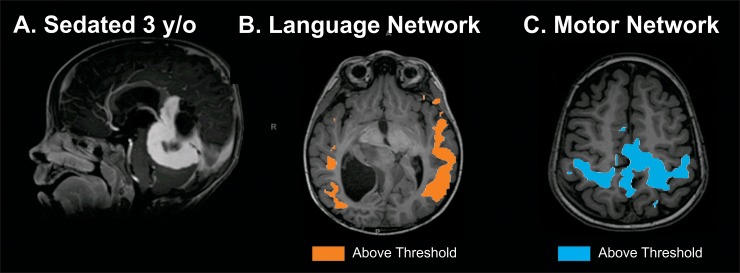
Functional magnetic resonance imaging (fMRI) is an important tool for pre-surgical evaluation of eloquent cortex. Classic task-based paradigms require patient participation and individual imaging sequence acquisitions for each functional domain that is being assessed. Resting state fMRI (rs-fMRI), however, enables functional localization without patient participation and can evaluate numerous functional domains with a single imaging session. To date, post-processing of this resting state data has been resource intensive, which limits its widespread application for routine clinical use. Through a novel automated algorithm and advanced imaging IT structure, we report the clinical application and the large-scale integration of rs-fMRI into routine neurosurgical practice. One hundred and ninety one consecutive patients underwent a 3T rs-fMRI, 83 of whom also underwent both motor and language task-based fMRI. Data were processed using a novel, automated, multi-layer perceptron algorithm and integrated into stereotactic navigation using a streamlined IT imaging pipeline. One hundred eighty-five studies were performed for intracranial neoplasm, 14 for refractory epilepsy and 33 for vascular malformations or other neurological disorders. Failure rate of rs-fMRI of 13% was significantly better than that for task-based fMRI (38.5%,) (p <0.001). In conclusion, at Washington University in St. Louis, rs-fMRI has become an integral part of standard imaging for neurosurgical planning. Resting state fMRI can be used in all patients, and due to its lower failure rate than task-based fMRI, it is useful for patients who are unable to cooperate with task-based studies.
Conflict of interest statement
Eric C. Leuthardt has ownership of stock in Neurolutions and Inner Cosmos. This does not alter our adherence to PLOS ONE policies on sharing data and materials (as detailed online in the guide for authors).
Figures
References
-
- Gulati S., Jakola A.S., Nerland U.S., Weber C., and Solheim O., The risk of getting worse: surgically acquired deficits, perioperative complications, and functional outcomes after primary resection of glioblastoma. World Neurosurg, 2011. 76(6): p. 572–9. doi: 10.1016/j.wneu.2011.06.014 - DOI - PubMed
-
- Lacroix M., Abi-Said D., Fourney D.R., Gokaslan Z.L., Shi W., DeMonte F., et al., A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg, 2001. 95(2): p. 190–8. doi: 10.3171/jns.2001.95.2.0190 - DOI - PubMed
-
- McGirt M.J., Mukherjee D., Chaichana K.L., Than K.D., Weingart J.D., and Quinones-Hinojosa A., Association of surgically acquired motor and language deficits on overall survival after resection of glioblastoma multiforme. Neurosurgery, 2009. 65(3): p. 463–9; discussion 469–70. doi: 10.1227/01.NEU.0000349763.42238.E9 - DOI - PubMed
-
- Ojemann G.A., Functional mapping of cortical language areas in adults. Intraoperative approaches. Advances in neurology, 1993. 63: p. 155–63. - PubMed
-
- Petrella J.R., Shah L.M., Harris K.M., Friedman A.H., George T.M., Sampson J.H., et al J.S., Preoperative functional MR imaging localization of language and motor areas: effect on therapeutic decision making in patients with potentially resectable brain tumors. Radiology, 2006. 240(3): p. 793–802. doi: 10.1148/radiol.2403051153 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
