

Improved empirical antibiotic treatment of sepsis after an educational intervention: the ABISS-Edusepsis study
- PMID: 29933756
- PMCID: PMC6013897
- DOI: 10.1186/s13054-018-2091-0
Improved empirical antibiotic treatment of sepsis after an educational intervention: the ABISS-Edusepsis study
Abstract
Background: Early appropriate antibiotic treatment is essential in sepsis. We aimed to evaluate the impact of a multifaceted educational intervention to improve antibiotic treatment. We hypothesized that the intervention would hasten and improve the appropriateness of empirical antibiotic administration, favor de-escalation, and decrease mortality.
Methods: We prospectively studied all consecutive patients with sepsis/septic shock admitted to 72 intensive care units (ICUs) throughout Spain in two 4-month periods (before and immediately after the 3-month intervention). We compared process-of-care variables (resuscitation bundle and time-to-initiation, appropriateness, and de-escalation of empirical antibiotic treatment) and outcome variables between the two cohorts. The primary outcome was hospital mortality. We analyzed the intervention's long-term impact in a subset of 50 ICUs.
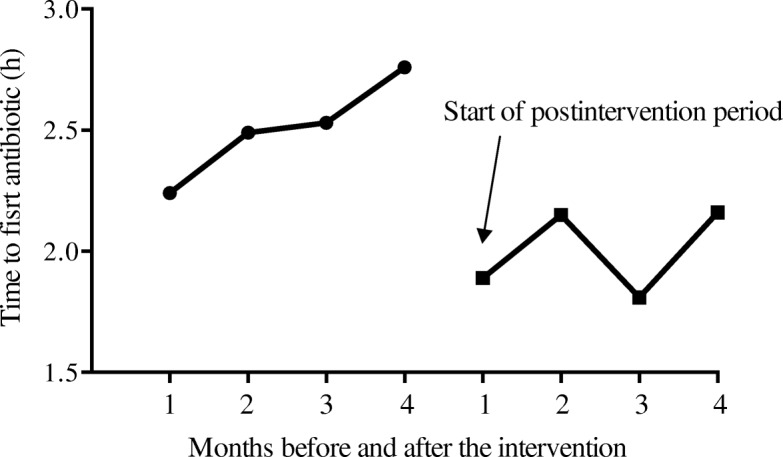
Results: We included 2628 patients (age 64.1 ± 15.2 years; men 64.0%; Acute Physiology and Chronic Health Evaluation (APACHE) II, 22.0 ± 8.1): 1352 in the preintervention cohort and 1276 in the postintervention cohort. In the postintervention cohort, the mean (SD) time from sepsis onset to empirical antibiotic therapy was lower (2.0 (2.7) vs. 2.5 (3.6) h; p = 0.002), the proportion of inappropriate empirical treatments was lower (6.5% vs. 8.9%; p = 0.024), and the proportion of patients in whom antibiotic treatment was de-escalated was higher (20.1% vs. 16.3%; p = 0.004); the expected reduction in mortality did not reach statistical significance (29.4% in the postintervention cohort vs. 30.5% in the preintervention cohort; p = 0.544). Gains observed after the intervention were maintained in the long-term follow-up period.
Conclusions: Despite advances in sepsis treatment, educational interventions can still improve the delivery of care; further improvements might also improve outcomes.
Keywords: De-escalation; Hospital mortality; Quality improvement; Sepsis; Septic shock; Timing of antibiotics.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by our institutional review board (reference 2,011,521) and the ethics committees at each participating center approved the study protocol and waived the need for informed consent because the intervention was a quality improvement program and patients’ anonymity was guaranteed.
Consent for publication
Not applicable.
Competing interests
AA received funding for himself from Grifols, Lilly Foundation, and Fisher & Paykel. Other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
