

Simulation-based training for trauma resuscitation among ACS TQIP-Pediatric centers: Understanding prevalence of use, associated center characteristics, training factors, and implementation barriers
- PMID: 29934123
- PMCID: PMC7169990
- DOI: 10.1016/j.amjsurg.2018.06.009
Simulation-based training for trauma resuscitation among ACS TQIP-Pediatric centers: Understanding prevalence of use, associated center characteristics, training factors, and implementation barriers
Abstract
Background: Simulation-based training (SBT) for pediatric trauma resuscitation can improve team performance. The purpose of this study was to describe the nationwide trend in SBT use and barriers to SBT implementation.
Methods: Trauma centers that participated in ACS TQIP Pediatric in 2016 (N = 125) were surveyed about SBT use. Center characteristics and reported implementation barriers were compared between centers using and not using SBT.
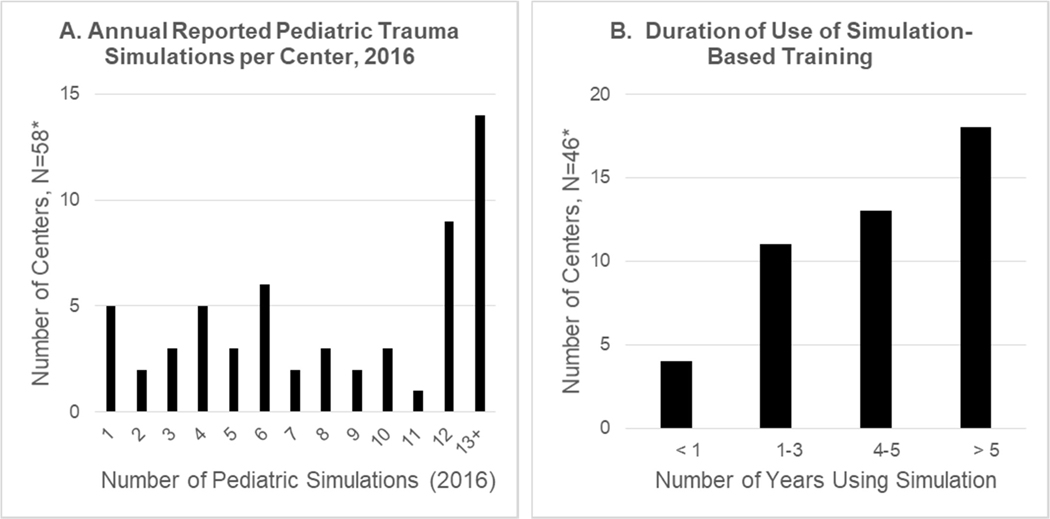
Results: Survey response rate was 75% (94/125) with 78% (73/94) reporting SBT use. The frequency of pediatric SBT use increased from 2014 to 2016 (median 5.5 vs 6.5 annual sessions, p < 0.01). Funding barriers were negatively associated with number of annual SBT sessions (r ≤ -0.34, p < 0.05). Centers not using SBT reported lack of technical expertise (p = 0.01) and lack of data supporting SBT (p = 0.03) as significant barriers.
Conclusions: Simulation use increased from 2014 to 2016, but significant barriers to implementation exist. Strategies to share resources and decrease costs may improve usage.
Level of evidence: Level 3, epidemiological.
Keywords: Barriers; Implementation; Pediatric trauma; Simulation; Simulation-based training; Trauma resuscitation.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
References
-
- Borse N, Sleet DA. CDC Childhood Injury Report: Patterns of Unintentional Injuries Among 0- to 19-Year Olds in the United States, 2000–2006. Fam Community Health. 2009;32:189. - PubMed
-
- Borse NN, Gilchrist J, Dellinger AM, et al. Unintentional childhood injuries in the United States: key findings from the CDC childhood injury report. J Saf Res. 2009;40:71–74. - PubMed
-
- National Center for Injury Prevention and Control, CDC using WISQARS. https://www.cdc.gov/injury/wisqars/LeadingCauses.html; 2017. Accessed 17 May 2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
