

Beta-blocker use and cardiovascular event risk in patients with heart failure with preserved ejection fraction
- PMID: 29934526
- PMCID: PMC6015007
- DOI: 10.1038/s41598-018-27799-y
Beta-blocker use and cardiovascular event risk in patients with heart failure with preserved ejection fraction
Abstract
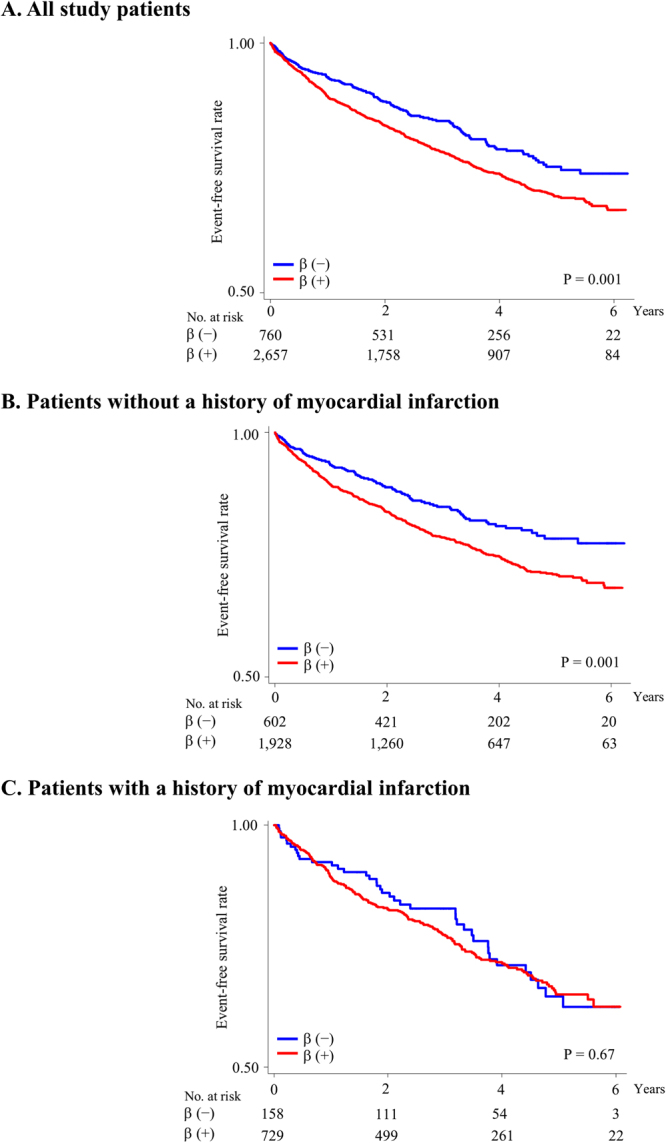
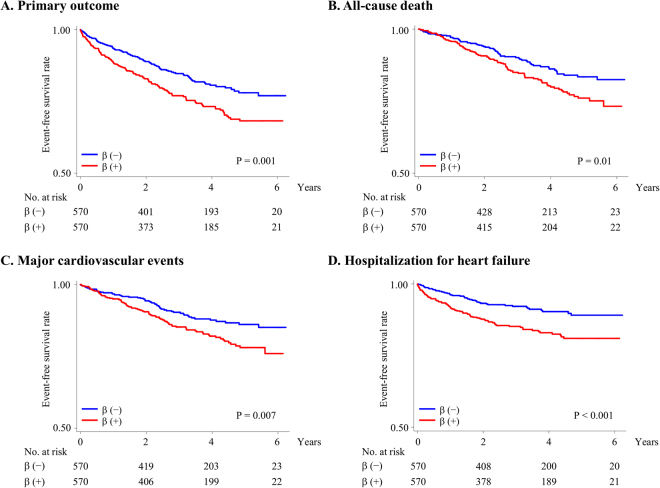
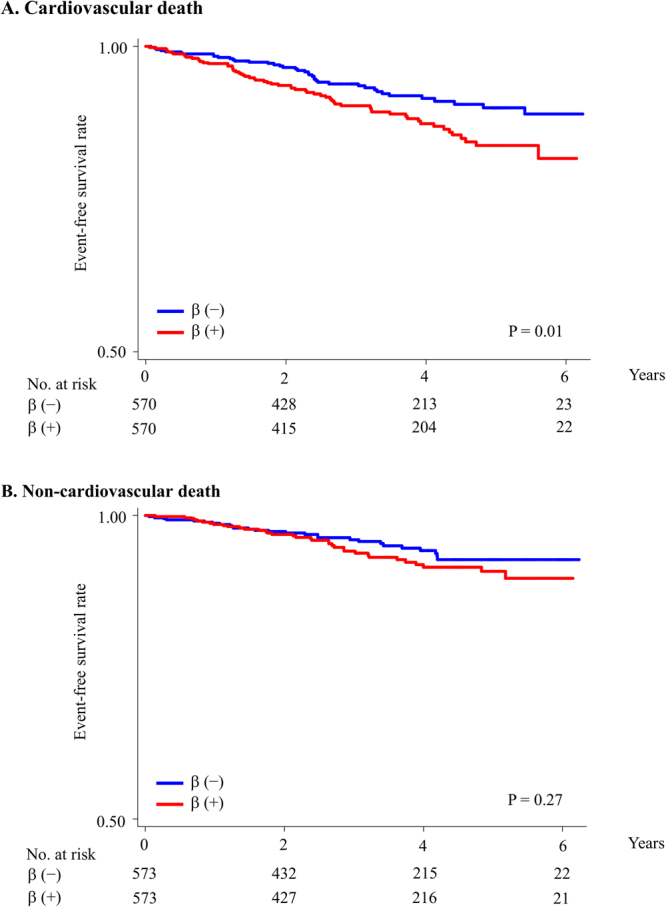
To assess whether beta-blocker use is associated with cardiovascular events and mortality in patients with heart failure with preserved ejection fraction (HFpEF), this study analyzed the Treatment of Preserved Cardiac Function Heart Failure with an Aldosterone Antagonist (TOPCAT) trial data using Cox proportional hazard models. Adjusted HRs for composite cardiovascular events in all patients and in patients without previous MI were significantly higher for those on beta-blockers than for those not on beta-blockers (Hazard ratio [HR] for all patients 1.23, 95% confidence interval [95% CI] 1.02-1.49; HR for patients without previous MI 1.35, 95% CI 1.08-1.70), whereas that for patients with previous MI was not significantly different (HR 1.06, 95% CI 0.74-1.54). Additionally, cardiovascular event risk in propensity score-matched patients without previous MI was significantly higher in those on beta-blockers than in those not on beta-blockers. Risks of all-cause death, major cardiovascular events, and heart failure hospitalization were significantly higher in those on beta-blockers than in those not on beta-blockers. Beta-blocker use in HFpEF patients, particularly those without previous MI, was associated with increased risk of unfavorable cardiovascular events.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
