

Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery
- PMID: 29934987
- PMCID: PMC6513198
- DOI: 10.1002/14651858.CD009621.pub3
Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery
Update in
-
Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery.Cochrane Database Syst Rev. 2020 Mar 11;3(3):CD009621. doi: 10.1002/14651858.CD009621.pub4. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2023 Jun 19;6:CD009621. doi: 10.1002/14651858.CD009621.pub5. PMID: 32157697 Free PMC article. Updated.
Abstract
Background: Postoperative pancreatic fistula is one of the most frequent and potentially life-threatening complications following pancreatic resections. Fibrin sealants are introduced to reduce postoperative pancreatic fistula by some surgeons. However, the use of fibrin sealants during pancreatic surgery is controversial. This is an update of a Cochrane Review last published in 2016.
Objectives: To assess the safety, effectiveness, and potential adverse effects of fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery.
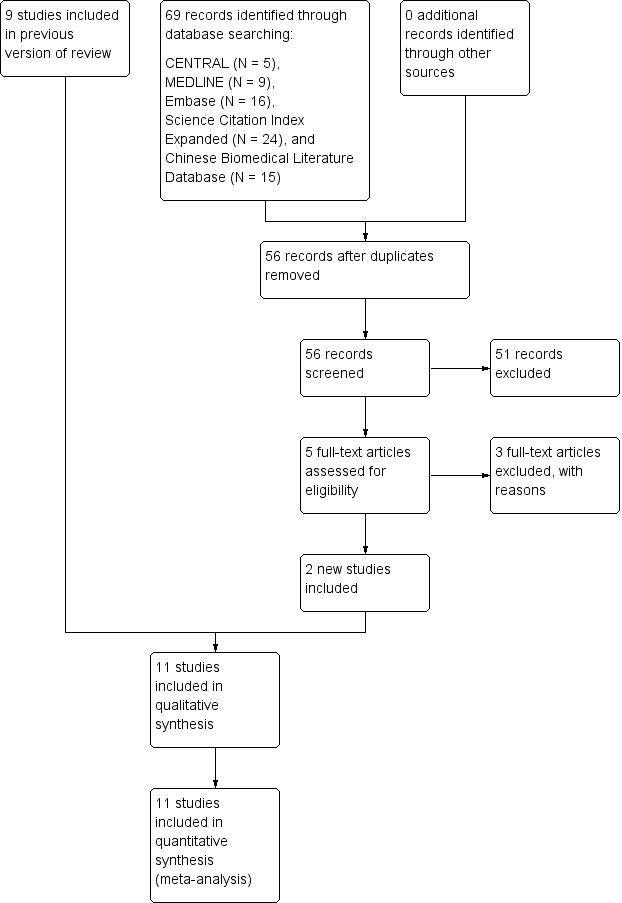
Search methods: We searched trial registers and the following biomedical databases: the Cochrane Library (2018, Issue 4), MEDLINE (1946 to 12 April 2018), Embase (1980 to 12 April 2018), Science Citation Index Expanded (1900 to 12 April 2018), and Chinese Biomedical Literature Database (CBM) (1978 to 12 April 2018).
Selection criteria: We included all randomized controlled trials that compared fibrin sealant (fibrin glue or fibrin sealant patch) versus control (no fibrin sealant or placebo) in people undergoing pancreatic surgery.
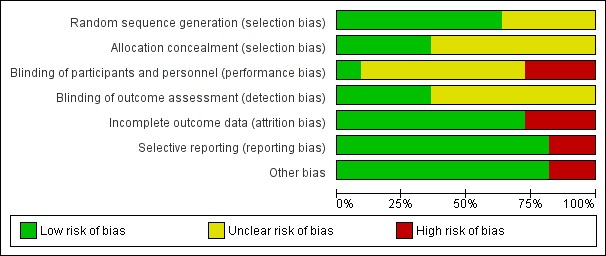
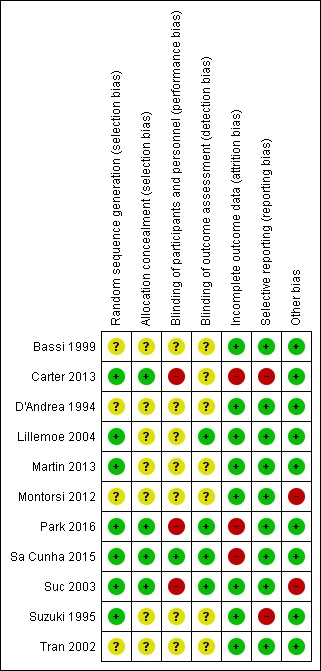
Data collection and analysis: Two review authors independently identified the trials for inclusion, collected the data, and assessed the risk of bias. We performed the meta-analyses using Review Manager 5. We calculated the risk ratio (RR) for dichotomous outcomes (or a Peto odds ratio (OR) for very rare outcomes), and the mean difference (MD) for continuous outcomes, with 95% confidence intervals (CIs).
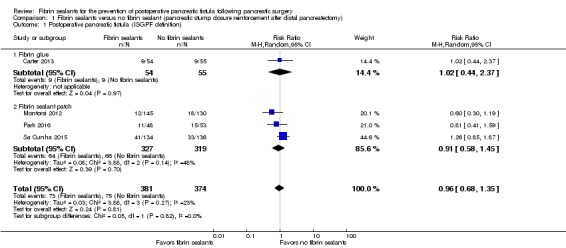
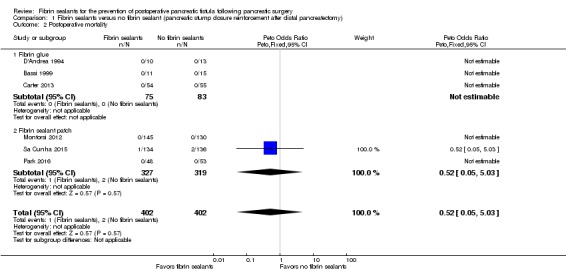
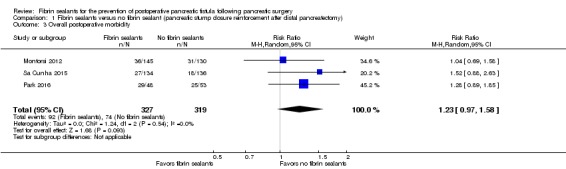
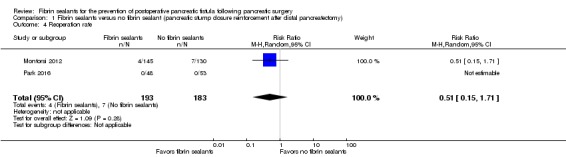
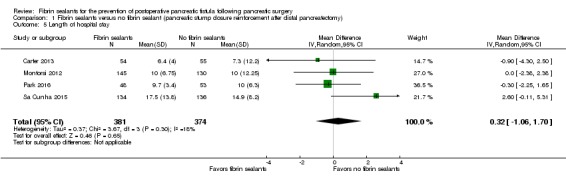
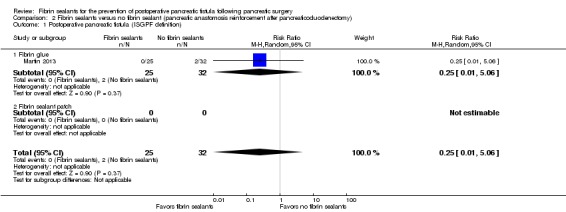
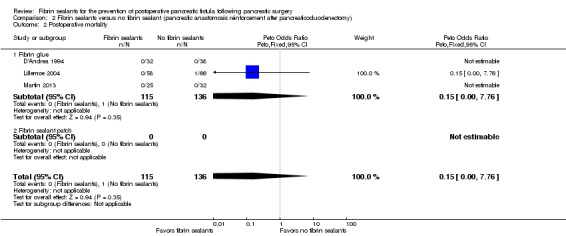
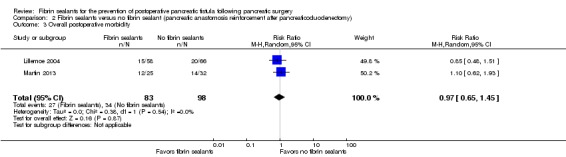
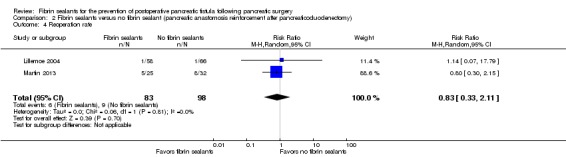
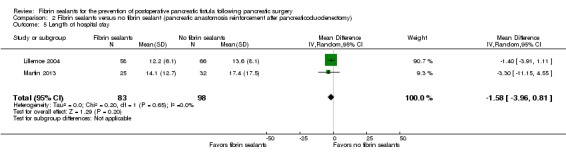
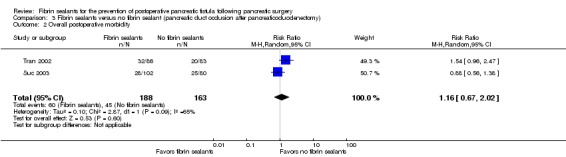
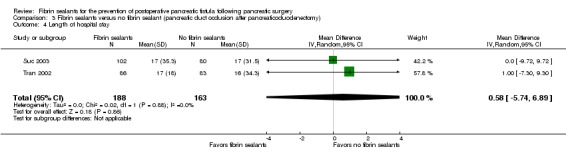
Main results: We included 11 studies involving 1462 participants in the review.Application of fibrin sealants to pancreatic stump closure reinforcement after distal pancreatectomyWe included seven studies involving 860 participants: 428 were randomized to the fibrin sealant group and 432 to the control group after distal pancreatectomy. Fibrin sealants may lead to little or no difference in postoperative pancreatic fistula (fibrin sealant 19.3%; control 20.1%; RR 0.96, 95% CI 0.68 to 1.35; 755 participants; four studies; low-quality evidence). Fibrin sealants may also lead to little or no difference in postoperative mortality (0.3% versus 0.5%; Peto OR 0.52, 95% CI 0.05 to 5.03; 804 participants; six studies; low-quality evidence), or overall postoperative morbidity (28.5% versus 23.2%; RR 1.23, 95% CI 0.97 to 1.58; 646 participants; three studies; low-quality evidence). We are uncertain whether fibrin sealants reduce reoperation rate (2.0% versus 3.8%; RR 0.51, 95% CI 0.15 to 1.71; 376 participants; two studies; very low-quality evidence). There is probably little or no difference in length of hospital stay between the groups (12.1 days versus 11.4 days; MD 0.32 days, 95% CI -1.06 to 1.70; 755 participants; four studies; moderate-quality evidence). The studies did not report serious adverse events, quality of life, or cost effectiveness.Application of fibrin sealants to pancreatic anastomosis reinforcement after pancreaticoduodenectomyWe included three studies involving 251 participants: 115 were randomized to the fibrin sealant group and 136 to the control group after pancreaticoduodenectomy. We are uncertain whether fibrin sealants reduce postoperative pancreatic fistula (1.6% versus 6.2%; RR 0.25, 95% CI 0.01 to 5.06; 57 participants; one study; very low-quality evidence). Fibrin sealants may lead to little or no difference in postoperative mortality (0.1% versus 0.7%; Peto OR 0.15, 95% CI 0.00 to 7.76; 251 participants; three studies; low-quality evidence) or length of hospital stay (12.8 days versus 14.8 days; MD -1.58 days, 95% CI -3.96 to 0.81; 181 participants; two studies; low-quality evidence). We are uncertain whether fibrin sealants reduce overall postoperative morbidity (33.7% versus 34.7%; RR 0.97, 95% CI 0.65 to 1.45; 181 participants; two studies; very low-quality evidence), or reoperation rate (7.6% versus 9.2%; RR 0.83, 95% CI 0.33 to 2.11; 181 participants; two studies, very low-quality evidence). The studies did not report serious adverse events, quality of life, or cost effectiveness.Application of fibrin sealants to pancreatic duct occlusion after pancreaticoduodenectomyWe included two studies involving 351 participants: 188 were randomized to the fibrin sealant group and 163 to the control group after pancreaticoduodenectomy. Fibrin sealants may lead to little or no difference in postoperative mortality (8.4% versus 6.1%; Peto OR 1.41, 95% CI 0.63 to 3.13; 351 participants; two studies; low-quality evidence) or length of hospital stay (17.0 days versus 16.5 days; MD 0.58 days, 95% CI -5.74 to 6.89; 351 participants; two studies; low-quality evidence). We are uncertain whether fibrin sealants reduce overall postoperative morbidity (32.0% versus 27.6%; RR 1.16, 95% CI 0.67 to 2.02; 351 participants; two studies; very low-quality evidence), or reoperation rate (13.6% versus 16.0%; RR 0.85, 95% CI 0.52 to 1.41; 351 participants; two studies; very low-quality evidence). Serious adverse events were reported in one study: more participants developed diabetes mellitus when fibrin sealants were applied to pancreatic duct occlusion, both at three months' follow-up (33.7% fibrin sealant group versus 10.8% control group; 29 participants versus 9 participants) and 12 months' follow-up (33.7% fibrin sealant group versus 14.5% control group; 29 participants versus 12 participants). The studies did not report postoperative pancreatic fistula, quality of life, or cost effectiveness.
Authors' conclusions: Based on the current available evidence, fibrin sealants may have little or no effect on postoperative pancreatic fistula in people undergoing distal pancreatectomy. The effects of fibrin sealants on the prevention of postoperative pancreatic fistula are uncertain in people undergoing pancreaticoduodenectomy.
Conflict of interest statement
Junhua Gong: none known.
SH: none known.
YC: none known.
NC: none known.
Jianping Gong: none known.
ZZ: none known.
Figures


Update of
-
Fibrin sealants for the prevention of postoperative pancreatic fistula following pancreatic surgery.Cochrane Database Syst Rev. 2016 Feb 15;2:CD009621. doi: 10.1002/14651858.CD009621.pub2. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2018 Jun 23;6:CD009621. doi: 10.1002/14651858.CD009621.pub3. PMID: 26876721 Updated.
References
References to studies included in this review
-
- Bassi C, Butturini G, Falconi M, Salvia RNS, Caldiron E, Talamini G, et al. Prospective randomised pilot study of management of the pancreatic stump following distal resection. HPB : the official journal of the International Hepato Pancreato Biliary Association 1999;1(4):203‐7.
-
- Carter TI, Fong ZV, Hyslop T, Lavu H, Tan WP, Hardacre J, et al. A dual‐institution randomized controlled trial of remnant closure after distal pancreatectomy: does the addition of a falciform patch and fibrin glue improve outcomes?. Journal of Gastrointestinal Surgery 2013;17(1):102‐9. - PubMed
-
- D'Andrea AA, Costantino V, Sperti C, Pedrazzoli S. Human fibrin sealant in pancreatic surgery: it is useful in preventing fistulas? A prospective randomized study. Italian Journal of Gastroenterology 1994;26(6):283‐6. - PubMed
-
- Lillemoe KD, Cameron JL, Kim MP, Campbell KA, Sauter PK, Coleman JA, et al. Does fibrin glue sealant decrease the rate of pancreatic fistula after pancreaticoduodenectomy? Results of a prospective randomized trial. Journal of Gastrointestinal Surgery 2004;8(7):772‐4. - PubMed
References to studies excluded from this review
-
- Mita K, Ito H, Murabayashi R, Asakawa H, Nabetani M, Kamasako A, Koizumi K, et al. Use of a fibrinogen/thrombin‐based collagen fleece (TachoComb, TachoSil) with a stapled closure to prevent pancreatic fistula formation following distal pancreatectomy. Surgical Innovation 2015;22(6):601‐5. - PubMed
-
- Ohwada S, Ogawa T, Tanahashi Y, Nakamura S, Takeyoshi I, Ohya T, et al. Fibrin glue sandwich prevents pancreatic fistula following distal pancreatectomy. World Journal of Surgery 1998;22(5):494‐8. - PubMed
-
- Rehman S, Jaques BC. Does a fibrin glue sealant decrease post‐operative pancreatic fistulae after pancreaticoduodenectomy; a single centre comparative study in 100 consecutive patients undergoing Whipple's procedure by a single surgeon. HPB: the official journal of the International Hepato Pancreato Biliary Association. Manchester: Elsevier, 2016; Vol. 18:e836‐e837.
- Rehman S, Jaques BC. Does fibrin glue sealant used during pancreaticoduodenectomy reduce post‐operative complication? Audit of 100 consecutive patients undergoing Whipple's procedure by a single surgeon. Journal of the Pancreas 2016;17(2):189‐95.
-
- Silvestri S, Franchello A, Gonella F, Deiro G, Campra D, Cassine D, et al. Role of TachoSil® in distal pancreatectomy: a single center experience. Minerva Chirurgica 2015;70(3):175‐80. - PubMed
Additional references
-
- Anderson KE, Mack TM, Silverman DT. Cancer of the pancreas. In: Schottenfeld D, Fraumeni JF Jr editor(s). Cancer Epidemiology and Prevention. 3rd Edition. New York: Oxford University Press, 2006:721‐63.
-
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005;138(1):8‐13. - PubMed
-
- Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 2017;161(3):584‐91. - PubMed
-
- Braganza JM, Lee SH, McCloy RF, McMahon MJ. Chronic pancreatitis. Lancet 2011;377(9772):1184–97. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous