

Pathogen colonization of the gastrointestinal microbiome at intensive care unit admission and risk for subsequent death or infection
- PMID: 29936583
- PMCID: PMC6309661
- DOI: 10.1007/s00134-018-5268-8
Pathogen colonization of the gastrointestinal microbiome at intensive care unit admission and risk for subsequent death or infection
Abstract
Purpose: Loss of colonization resistance within the gastrointestinal microbiome facilitates the expansion of pathogens and has been associated with death and infection in select populations. We tested whether gut microbiome features at the time of intensive care unit (ICU) admission predict death or infection.
Methods: This was a prospective cohort study of medical ICU adults. Rectal surveillance swabs were performed at admission, selectively cultured for vancomycin-resistant Enterococcus (VRE), and assessed using 16S rRNA gene sequencing. Patients were followed for 30 days for death or culture-proven bacterial infection.
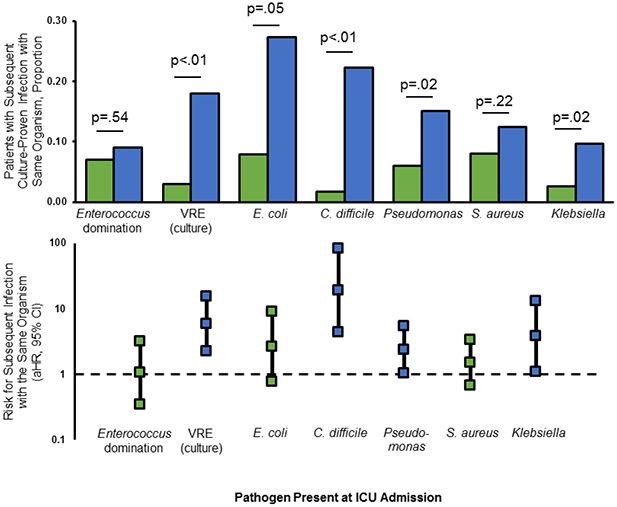
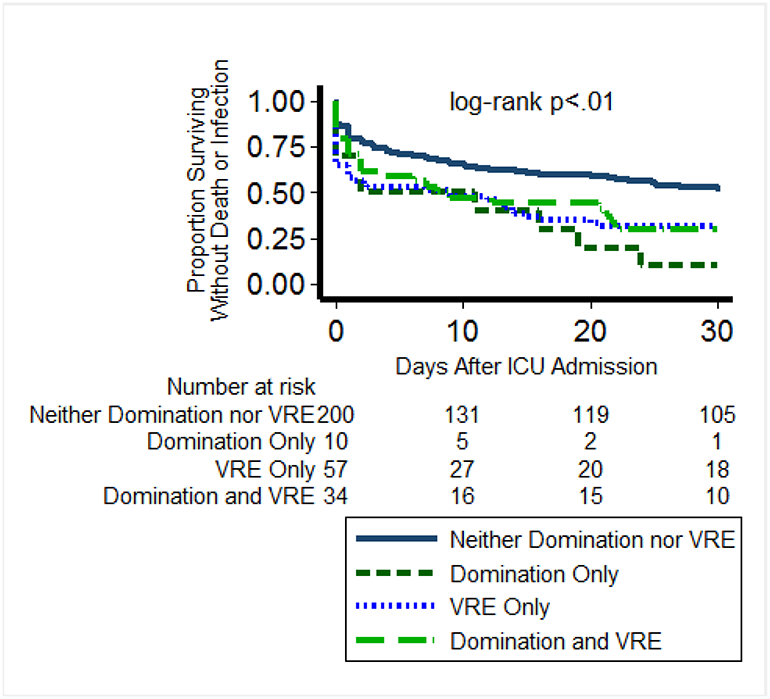
Results: Of 301 patients, 123 (41%) developed culture-proven infections and 76 (25%) died. Fecal biodiversity (Shannon index) did not differ based on death or infection (p = 0.49). The presence of specific pathogens at ICU admission was associated with subsequent infection with the same organism for Escherichia coli, Pseudomonas spp., Klebsiella spp., and Clostridium difficile, and VRE at admission was associated with subsequent Enterococcus infection. In a multivariable model adjusting for severity of illness, VRE colonization and Enterococcus domination (≥ 30% 16S reads) were both associated with death or all-cause infection (aHR 1.46, 95% CI 1.06-2.00 and aHR 1.47, 95% CI 1.00-2.19, respectively); among patients without VRE colonization, Enterococcus domination was associated with excess risk of death or infection (aHR 2.13, 95% CI 1.06-4.29).
Conclusions: Enterococcus status at ICU admission was associated with risk for death or all-cause infection, and rectal carriage of common ICU pathogens predicted specific infections. The gastrointestinal microbiome may have a role in risk stratification and early diagnosis of ICU infections.
Keywords: Colonization resistance; Critical care; Microbiome; Mortality; Nosocomial infection; Vancomycin-resistant Enterococcus.
Conflict of interest statement
Conflicts of interest
None of the authors have conflicts of interest.
Figures
Comment in
-
The gut microbiota of critically ill patients: first steps in an unexplored world.Intensive Care Med. 2018 Sep;44(9):1561-1564. doi: 10.1007/s00134-018-5309-3. Epub 2018 Jul 14. Intensive Care Med. 2018. PMID: 30008112 No abstract available.
-
Microbiota in ICU, not only a gut problem.Intensive Care Med. 2019 May;45(5):733-737. doi: 10.1007/s00134-018-05516-7. Epub 2019 Jan 22. Intensive Care Med. 2019. PMID: 30671622 No abstract available.
References
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K, Investigators EIGo (2009). International study of the prevalence and outcomes of infection in intensive care units. JAMA 302:2323–9 - PubMed
-
- Garrouste-Orgeas M, Timsit JF, Tafflet M, Misset B, Zahar JR, Soufir L, Lazard T, Jamali S, Mourvillier B, Cohen Y, De Lassence A, Azoulay E, Cheval C, Descorps-Declere A, Adrie C, Costa de Beauregard MA, Carlet J, Group OS (2006). Excess risk of death from intensive care unit-acquired nosocomial bloodstream infections: a reappraisal. Clin Infect Dis 42:1118–26 - PubMed
-
- Donskey CJ (2006). Antibiotic regimens and intestinal colonization with antibiotic-resistant gram-negative bacilli. Clin Infect Dis 43 Suppl 2:S62–9 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
