

Osteolytic lesions (brown tumors) of primary hyperparathyroidism misdiagnosed as multifocal giant cell tumor of the distal ulna and radius: a case report
- PMID: 29936913
- PMCID: PMC6016128
- DOI: 10.1186/s13256-018-1723-y
Osteolytic lesions (brown tumors) of primary hyperparathyroidism misdiagnosed as multifocal giant cell tumor of the distal ulna and radius: a case report
Abstract
Background: Brown tumors represent a rare clinical manifestation reported in approximately 3% of patients with primary hyperparathyroidism and correspond to radiologically osteolytic lesions with well-defined borders in different parts of the skeleton.
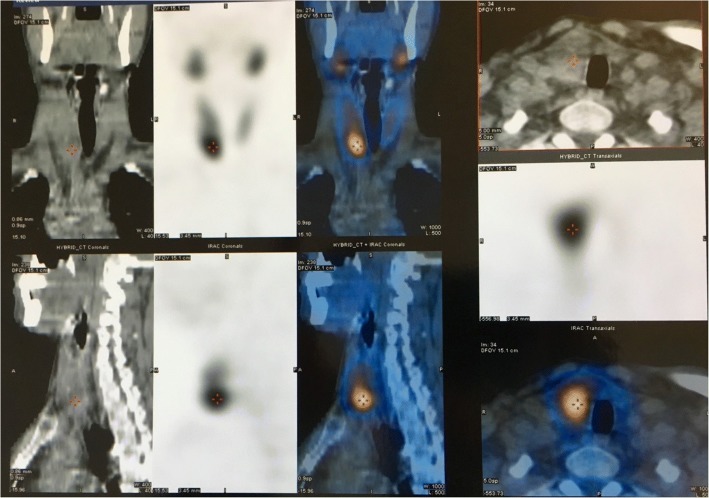
Case presentation: We report the case of a 53-year-old white man who presented to our hospital with osteolytic lesions of his distal ulna and radius, causing pain and swelling of 2-month duration. A subsequent biopsy revealed histological features consistent with giant cell tumor and a complete resection of his distal ulna was followed, along with curettage and cementoplasty of the distal radial metaphysis. Two weeks later, he was re-admitted with diffuse musculoskeletal soreness, anorexia, constipation, nausea, and localized abdominal pain and multiple osteolytic lesions on plain radiographs. A histopathological examination of the ulna and radius specimens showed similar findings and, given the multifocality, brown tumors related to primary or secondary hyperparathyroidism was included in the differential diagnosis. A laboratory examination showed high total serum calcium (14.5 mg/dl) and low serum phosphorus and 25-hydroxyvitamin D levels. Primary hyperparathyroidism was suspected and confirmed by the elevated parathyroid hormone levels of 1453 pg/mL. At radiological work-up, using computed tomography, ultrasonography, and parathyroid subtraction technetium-99m sestamibi scintigraphy, a 4.5 × 2.5 × 3.2 cm mass emanating from the right lobe of his thyroid gland was detected, displaying extensive uptake in the right lower parathyroid gland. After appropriate medical support including hyperhydration and high doses of diuretics and diphosphonates, his laboratory profile normalized and he underwent total thyroidectomy with removal of the parathyroid glands. Our patient is now recovering 12 months after surgery, with normal values of serum parathyroid hormone and calcium levels. The lytic bone lesions have almost disappeared and no other additional orthopedic intervention was necessary.
Conclusions: The present case report emphasizes the need of inclusion of brown tumors in the differential diagnosis of multifocal osteolytic bone lesions, in order to avoid harmful surgical interventions. Laboratory testing of serum phosphate, calcium levels, and parathyroid hormone levels should always be included in the routine survey of patients with multifocal osteolytic lesions.
Keywords: Brown tumor; Giant cell tumor; Parathyroid carcinoma; Primary hyperparathyroidism.
Conflict of interest statement
Ethics approval and consent to participate
No ethics approval is need for this type of manuscript, as the patient is still under medical care.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
