

Interaction of WBP2 with ERα increases doxorubicin resistance of breast cancer cells by modulating MDR1 transcription
- PMID: 29937544
- PMCID: PMC6048156
- DOI: 10.1038/s41416-018-0119-5
Interaction of WBP2 with ERα increases doxorubicin resistance of breast cancer cells by modulating MDR1 transcription
Abstract
Background: Surgery combined with new adjuvant chemotherapy is the primary treatment for early stage invasive and advanced stage breast cancer. Growing evidence indicates that patients with ERα-positive breast cancer show poor response to chemotherapeutics. However, ERα-mediated drug-resistant mechanisms remain unclear.
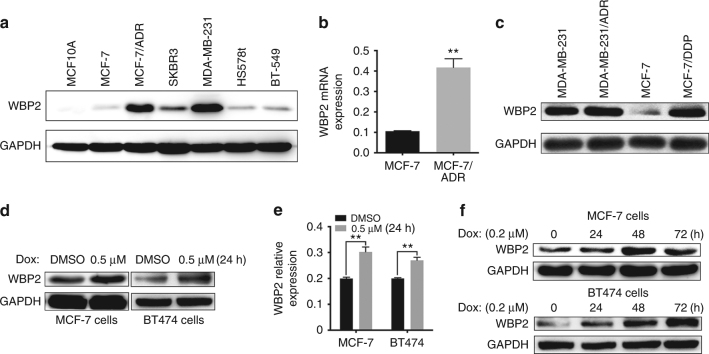
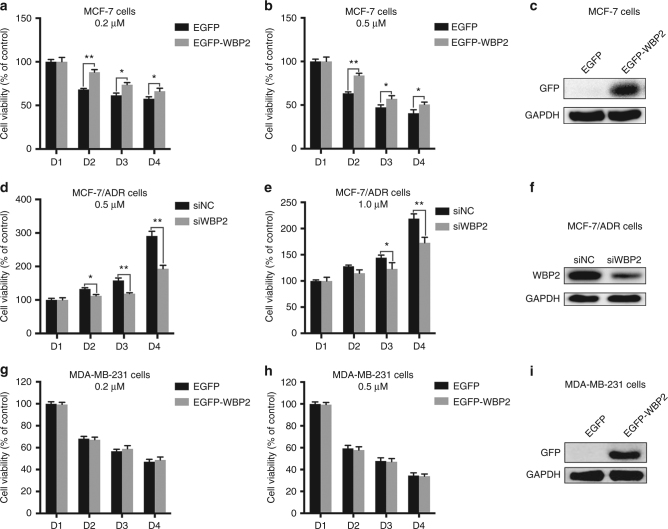
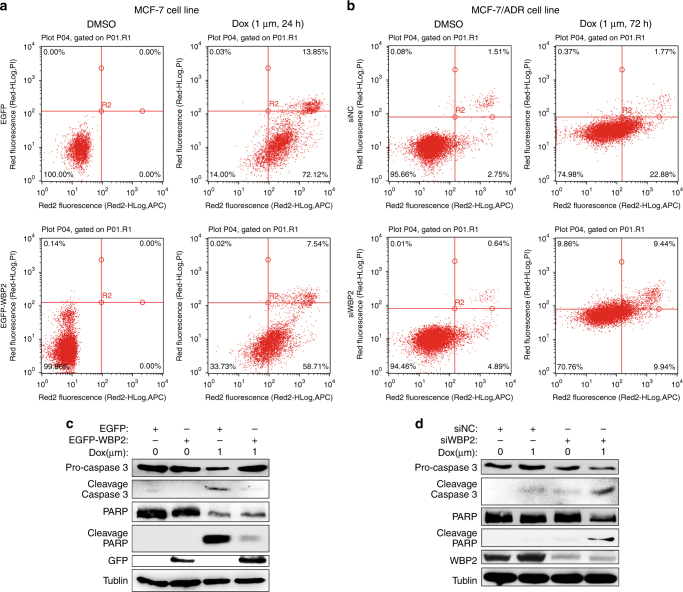
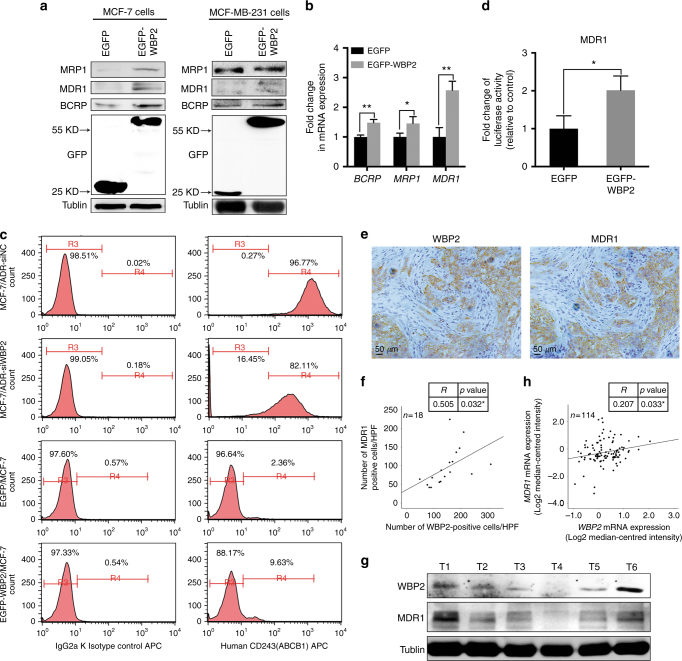
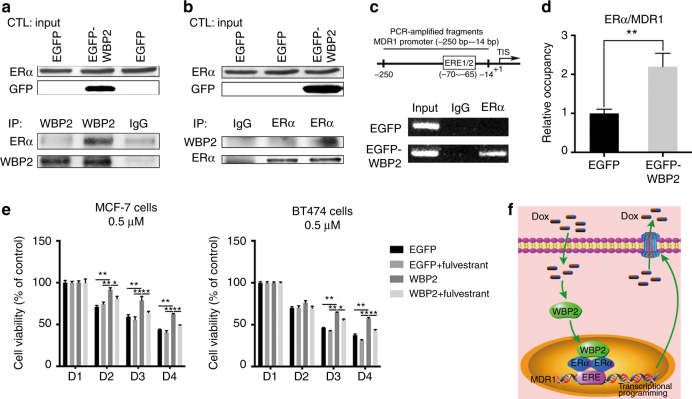
Methods: Levels of WW domain-binding protein 2 (WBP2) and drug-resistant gene were determined by western blotting and RT-PCR, respectively. Cell viability was measured by preforming MTT assay. CD243 expression and apoptosis rate were evaluated by flow cytometry. Interactions of WBP2/ERα and ERα/MDR1 were detected by co-immunoprecipitation and chromatin immunoprecipitation (ChIP) assay, respectively.
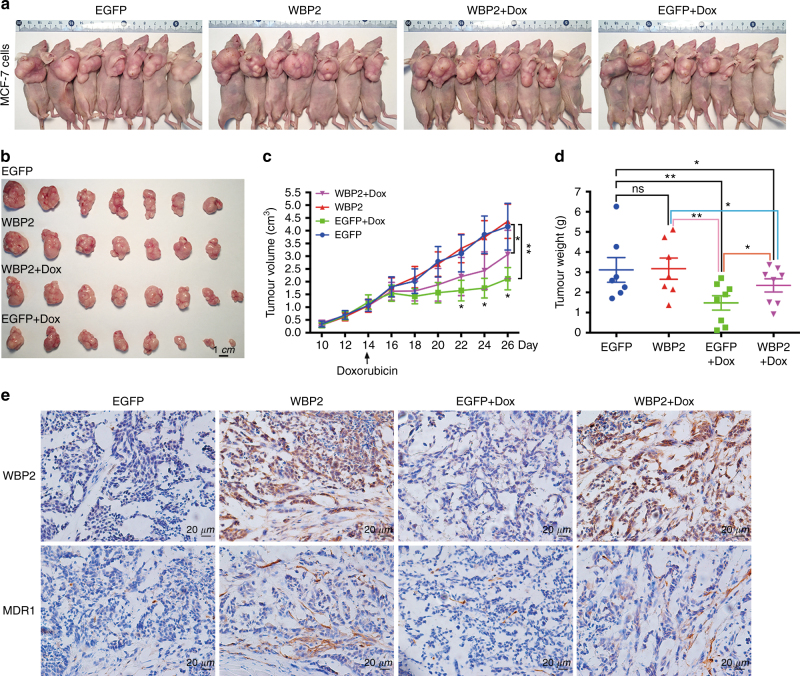
Results: There was an intrinsic link between WBP2 and ERα in drug-resistant cancer cells. Upregulation of WBP2 in MCF7 cells increased the chemoresistance to doxorubicin, while RNAi-mediated knockdown of WBP2 in MCF7/ADR cells sensitised the cancer cells to doxorubicin. Further investigation in in vitro and in vivo models demonstrated that WBP2 expression was directly correlated with MDR1, and WBP2 could directly modulate MDR1 transcription through binding to ERα, resulting in increased chemotherapy drug resistance.
Conclusions: Our finding provides a new mechanism for the chemotherapy response of ERα-positive breast tumours, and WBP2 might be a key molecule for developing new therapeutic strategies to treat chemoresistance in breast cancer patients.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
