

Amiloride resolves resistant edema and hypertension in a patient with nephrotic syndrome; a case report
- PMID: 29939487
- PMCID: PMC6016639
- DOI: 10.14814/phy2.13743
Amiloride resolves resistant edema and hypertension in a patient with nephrotic syndrome; a case report
Abstract
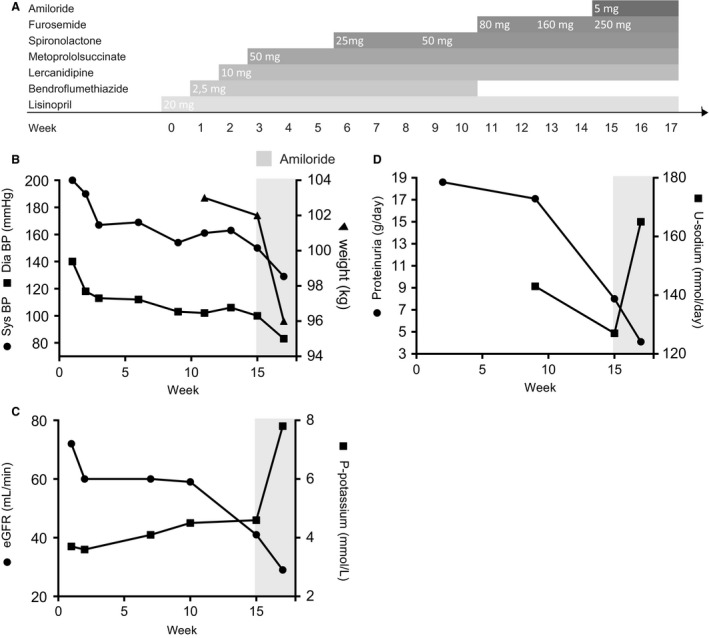
Sodium and fluid retention is a hallmark and a therapeutic challenge of the nephrotic syndrome (NS). Studies support the "overfill" theory of NS with pathophysiological proteolytic activation of the epithelial sodium channel (ENaC) which explains the common observation of suppressed renin -angiotensin system and poor therapeutic response to ACE inhibitors. Blockade of ENaC by the diuretic amiloride would be a rational intervention compared to the traditionally used loop diuretics. We describe a 38-year-old male patient with type1 diabetes who developed severe hypertension (200/140 mmHg), progressive edema (of at least 10 L), and overt proteinuria (18.5 g/24 h), despite combined administration of five antihypertensive drugs. Addition of amiloride (5 mg/day) to treatment resulted in resolution of edema, weight loss of 7 kg, reduction in blood pressure (150/100-125/81 mmHg), increased 24 h urinary sodium excretion (127-165 mmol/day), decreased eGFR (41-29 mL/min), and increased plasma potassium concentration (4.6-7.8 mmol/L). Blocking of ENaC mobilizes nephrotic edema and lowers blood pressure in NS. However, acute kidney injury and dangerous hyperkalemia is a potential risk if amiloride is added to multiple other antihypertensive medications as ACEi and spironolactone. The findings support that ENaC is active in NS and is a relevant target in adult NS patients.
Keywords: ENaC; plasmin; protease; proteinuria.
© 2018 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of The Physiological Society and the American Physiological Society.
Figures
Comment in
-
ENaC blockade in proteinuria-associated extracellular fluid volume overload - effective but risky.Physiol Rep. 2018 Sep;6(17):e13835. doi: 10.14814/phy2.13835. Physiol Rep. 2018. PMID: 30178569 Free PMC article. No abstract available.
Similar articles
-
Amiloride lowers blood pressure and attenuates urine plasminogen activation in patients with treatment-resistant hypertension.J Am Soc Hypertens. 2014 Dec;8(12):872-81. doi: 10.1016/j.jash.2014.09.019. J Am Soc Hypertens. 2014. PMID: 25492830 Clinical Trial.
-
Amiloride versus furosemide for the treatment of edema in patients with nephrotic syndrome: A pilot study (AMILOR).Acta Physiol (Oxf). 2024 Aug;240(8):e14183. doi: 10.1111/apha.14183. Epub 2024 Jun 1. Acta Physiol (Oxf). 2024. PMID: 38822593 Clinical Trial.
-
Aprotinin prevents proteolytic epithelial sodium channel (ENaC) activation and volume retention in nephrotic syndrome.Kidney Int. 2018 Jan;93(1):159-172. doi: 10.1016/j.kint.2017.07.023. Epub 2017 Oct 14. Kidney Int. 2018. PMID: 29042083
-
Perspectives on edema in childhood nephrotic syndrome.Am J Physiol Renal Physiol. 2015 Oct 1;309(7):F575-82. doi: 10.1152/ajprenal.00229.2015. Epub 2015 Aug 19. Am J Physiol Renal Physiol. 2015. PMID: 26290369 Review.
-
Mechanisms of sodium retention in nephrotic syndrome.Curr Opin Nephrol Hypertens. 2020 Mar;29(2):207-212. doi: 10.1097/MNH.0000000000000578. Curr Opin Nephrol Hypertens. 2020. PMID: 31789848 Review.
Cited by
-
Albumin is an interface between blood plasma and cell membrane, and not just a sponge.Clin Kidney J. 2021 Oct 5;15(4):624-634. doi: 10.1093/ckj/sfab194. eCollection 2022 Apr. Clin Kidney J. 2021. PMID: 35371452 Free PMC article.
-
Nephrotic Syndrome: Oedema Formation and Its Treatment With Diuretics.Front Physiol. 2019 Jan 15;9:1868. doi: 10.3389/fphys.2018.01868. eCollection 2018. Front Physiol. 2019. PMID: 30697163 Free PMC article. Review.
-
Oral Furosemide and Hydrochlorothiazide/Amiloride versus Intravenous Furosemide for the Treatment of Resistant Nephrotic Syndrome.J Clin Med. 2023 Nov 1;12(21):6895. doi: 10.3390/jcm12216895. J Clin Med. 2023. PMID: 37959360 Free PMC article.
-
Epithelial Na + Channels Function as Extracellular Sensors.Compr Physiol. 2024 Mar 29;14(2):1-41. doi: 10.1002/cphy.c230015. Compr Physiol. 2024. PMID: 39109974 Free PMC article. Review.
-
Regulating ENaC's gate.Am J Physiol Cell Physiol. 2020 Jan 1;318(1):C150-C162. doi: 10.1152/ajpcell.00418.2019. Epub 2019 Nov 13. Am J Physiol Cell Physiol. 2020. PMID: 31721612 Free PMC article. Review.
References
-
- Andersen, H. , Hansen P. B., Bistrup C., Nielsen F., Henriksen J. E., and Jensen B. L.. 2016. Significant natriuretic and antihypertensive action of the epithelial sodium channel blocker amiloride in diabetic patients with and without nephropathy. J. Hypertens. 34:1621–1629. - PubMed
-
- Bobrie, G. , Frank M., Azizi M., Peyrard S., Boutouyrie P., Chatellier G., et al. 2012. Sequential nephron blockade versus sequential renin‐angiotensin system blockade in resistant hypertension: a prospective, randomized, open blinded endpoint study. J. Hypertens. 30:1656–1664. - PubMed
-
- Bohnert, B. N. , Menacher M., Janessa A., Worn M., Schork A., Daiminger S., et al. 2017. Aprotinin prevents proteolytic epithelial sodium channel (ENaC) activation and volume retention in nephrotic syndrome. Kidney Int. 000:00. - PubMed
-
- Brown, E. A. , Markandu N. D., Roulston J. E., Jones B. E., Squires M., and MacGregor G. A.. 1982a. Is the renin‐angiotensin‐aldosterone system involved in the sodium retention in the nephrotic syndrome? Nephron 32:102–107. - PubMed
-
- Brown, E. A. , Markandu N. D., Sagnella G. A., Squires M., Jones B. E., and MacGregor G. A.. 1982b. Evidence that some mechanism other than the renin system causes sodium retention in nephrotic syndrome. Lancet (London, England) 2: 1237–1240. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
