

Arrest etiology among patients resuscitated from cardiac arrest
- PMID: 29940296
- PMCID: PMC6092216
- DOI: 10.1016/j.resuscitation.2018.06.024
Arrest etiology among patients resuscitated from cardiac arrest
Abstract
Introduction: Cardiac arrest etiology is often assigned according to the Utstein template, which differentiates medical (formerly "presumed cardiac") from other causes. These categories are poorly defined, contain within them many clinically distinct etiologies, and are rarely based on diagnostic testing. Optimal clinical care and research require more rigorous characterization of arrest etiology.
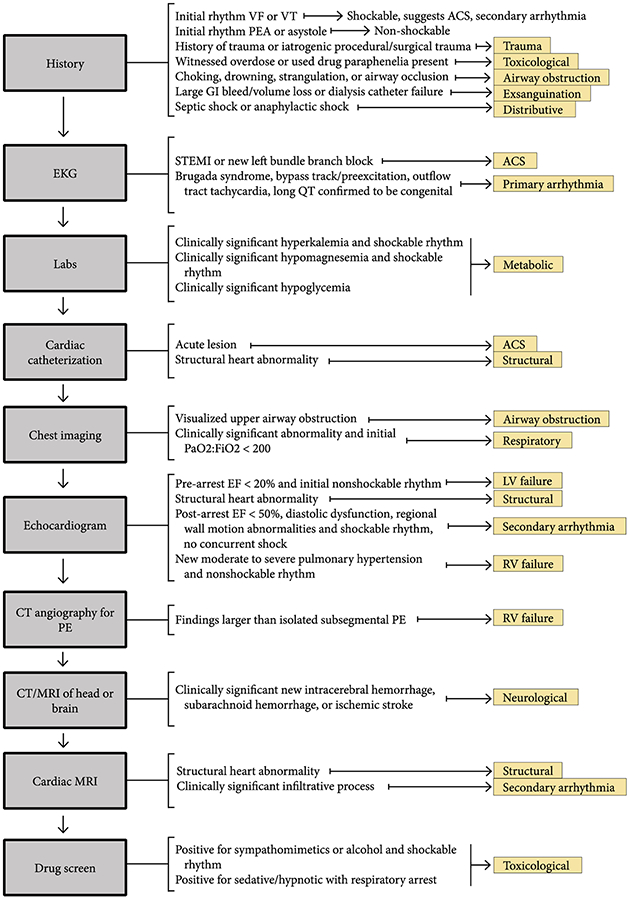
Methods: We developed a novel system to classify arrest etiology using a structured chart review of consecutive patients treated at a single center after in- or out-of-hospital cardiac arrest over four years. Two reviewers independently reviewed a random subset of 20% of cases to calculate inter-rater reliability. We used X2 and Kruskal-Wallis tests to compare baseline clinical characteristics and outcomes across etiologies.
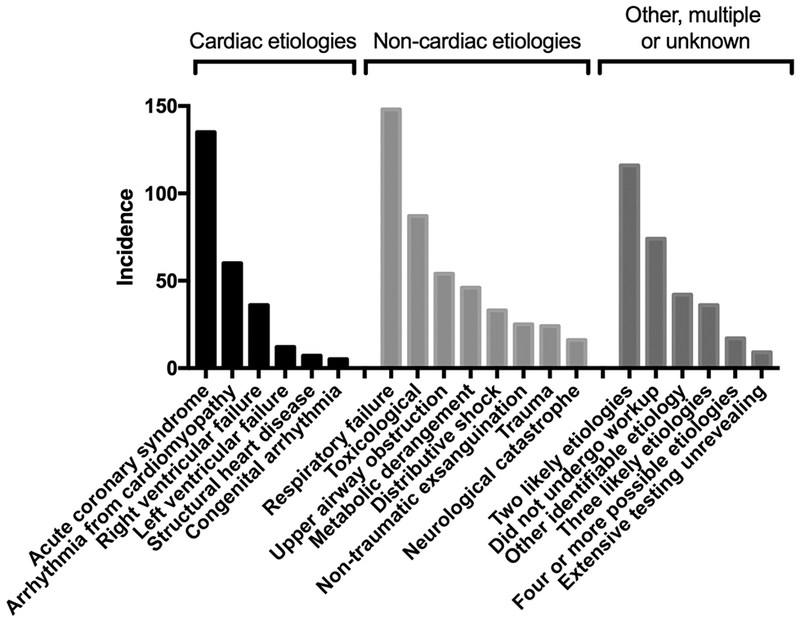
Results: We identified 14 principal arrest etiologies, and developed objective diagnostic criteria for each. Inter-rater reliability was high (kappa = 0.80). Median age of 986 included patients was 60 years, 43% were female and 71% arrested out-of-hospital. The most common etiology was respiratory failure (148 (15%)). A minority (255 (26%)) arrested due to cardiac causes. Only nine (1%) underwent a diagnostic workup that was unrevealing of etiology. Rates of awakening and survival to hospital discharge both differed across arrest etiologies, with survival ranging from 6% to 60% (both P < 0.001), and rates of favorable outcome ranging from 0% to 40% (P < 0.001). Timing and mechanism of death (e.g. multisystem organ failure or brain death) also differed significantly across etiologies.
Conclusions: Arrest etiology was identifiable in the majority cases via systematic chart review. "Cardiac" etiologies may be less common than previously thought. Substantial clinical heterogeneity exists across etiologies, suggesting previous classification systems may be insufficient.
Keywords: Cardiac arrest; Epidemiology; Etiology; Outcomes; Post-arrest.
Copyright © 2018 Elsevier B.V. All rights reserved.
Figures
References
-
- Perkins GD, Jacobs IG, Nadkarni VM, Berg RA, Bhanji F, Biarent D, Bossaert LL, Brett SJ, Chamberlain D, de Caen AR, Deakin CD, Finn JC, Grasner JT, Hazinski MF, Iwami T, Koster RW, Lim SH, Huei-Ming Ma M, McNally BF, Morley PT, Morrison LJ, Monsieurs KG, Montgomery W, Nichol G, Okada K, Eng Hock Ong M, Travers AH, Nolan JP, Utstein C, (2015) Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Circulation 132: 1286–1300 - PubMed
-
- Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Becker L, Bossaert L, Delooz HH, Dick WF, Eisenberg MS, et al. , (1991) Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionals from a task force of the American Heart Association, the European Resuscitation Council, the Heart and Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 84: 960–975 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
