

Survival of Immunoglobulins from Human Milk to Preterm Infant Gastric Samples at 1, 2, and 3 h Postprandial
- PMID: 29940583
- PMCID: PMC6217945
- DOI: 10.1159/000489387
Survival of Immunoglobulins from Human Milk to Preterm Infant Gastric Samples at 1, 2, and 3 h Postprandial
Abstract
Background: Human milk immunoglobulins (Ig) are an important support for the naïve infant immune system; yet the extent to which these proteins survive within the infant digestive tract, particularly for preterm infants, is poorly studied.
Objectives: Our objective was to evaluate the survival of human milk Igs in the preterm stomach across postprandial time.
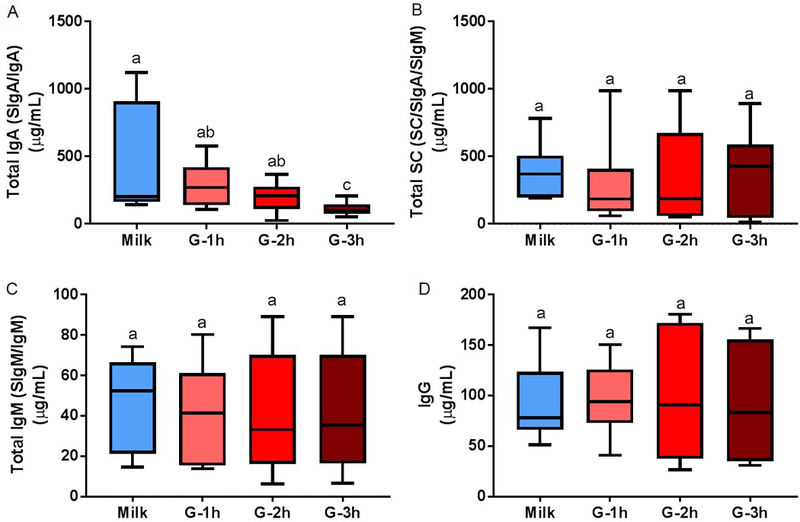
Methods: Human milk and infant gastric samples were collected from 11 preterm (23-32 weeks gestational age) mother-infant pairs within 7-98 days postnatal age. Preterm gastric samples were collected 1, 2, and 3 h after the beginning of the feeding. Samples were analyzed for concentration of total IgA (secretory IgA [SIgA]/IgA), total secretory component (SC/SIgA/SIgM), total IgM (SIgM/IgM), and IgG via enzyme-linked immunosorbent assay. Ig-chain fragment peptides were determined using peptidomic analysis. One-way analysis of variance with repeated measures followed by Tukey's multiple comparison tests was applied.
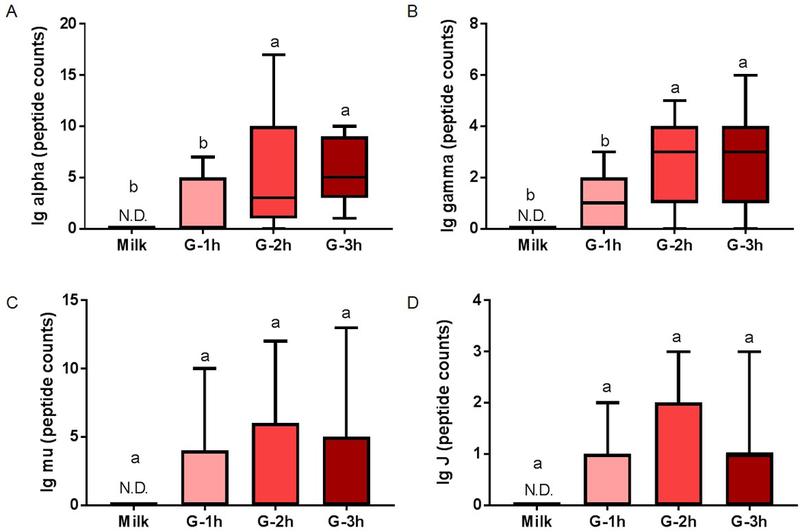
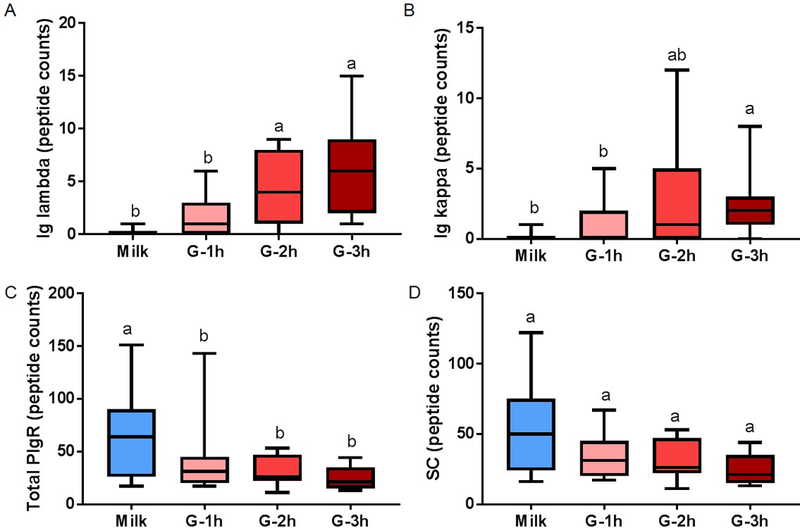
Results: Concentrations of total IgA were lower in the gastric contents at 3 h postprandial compared with human milk and gastric contents at 1 and 2 h. Human milk SC/SIgA/SIgM, IgG, and total IgM concentrations remained stable in the preterm stomach across postprandial time. Peptide counts from the Ig alpha-chain and the Ig gamma-chain increased in gastric contents from 1 to 2 h postprandial. Peptide counts from the human milk Ig-chain, Ig-chain, and SC were stable across postprandial time. These peptides from Ig-chains were not present in human milk but were released in the stomach due to their partial degradation.
Conclusions: Human milk total SC (SIgA/SC/SIgM), total IgM, and IgG survived mostly intact through the preterm infant stomach, while total IgA was -partially digested.
Keywords: Breast milk; Digestion; Gastric contents; Passive immunity; Peptidomic antibodies; Polymeric immunoglobulin receptor; Premature infants.
© 2018 S. Karger AG, Basel.
Conflict of interest statement
Disclosure Statement
There are no financial relationships or conflicts of interest to disclose.
Figures
References
-
- Oddy WH: Breastfeeding protects against illness and infection in infants and children: a review of the evidence. Breastfeed Rev 2001;9:11. - PubMed
-
- Van de Perre P: Transfer of antibody via mother’s milk. Vaccine 2003;21:3374–3376. - PubMed
-
- Goldman AS, Garza C, Nichols BL, Goldblum RM: Immunologic factors in human milk during the first year of lactation. J Pediatr 1982;100:563–567. - PubMed
-
- Chandra R: Immunoglobulin and protein levels in breast milk produced by mothers of preterm infants. Nutr Res 1982;2:27–30.
-
- Koenig Á, Diniz EMdA, Barbosa SFC, Vaz FAC: Immunologic factors in human milk: the effects of gestational age and pasteurization. J Hum Lact 2005;21:439–443. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
