

Analysis of the Risk Factors for Unfavorable Radiologic Outcomes after Fusion Surgery in Thoracolumbar Burst Fracture : What Amount of Postoperative Thoracolumbar Kyphosis Correction is Reasonable?
- PMID: 29940722
- PMCID: PMC6328790
- DOI: 10.3340/jkns.2017.0214
Analysis of the Risk Factors for Unfavorable Radiologic Outcomes after Fusion Surgery in Thoracolumbar Burst Fracture : What Amount of Postoperative Thoracolumbar Kyphosis Correction is Reasonable?
Abstract
Objective: The aims in the management of thoracolumbar spinal fractures are not only to restore vertebral column stability, but also to obtain acceptable alignment of the thoracolumbar junction (T-L junction) to prevent complications. However, insufficient surgical correction of the thoracolumbar spine would be likely to cause late progression of abnormal kyphosis. Therefore, we identified the surgical factors that affected unfavorable radiologic outcomes of the thoracolumbar spine after surgery.
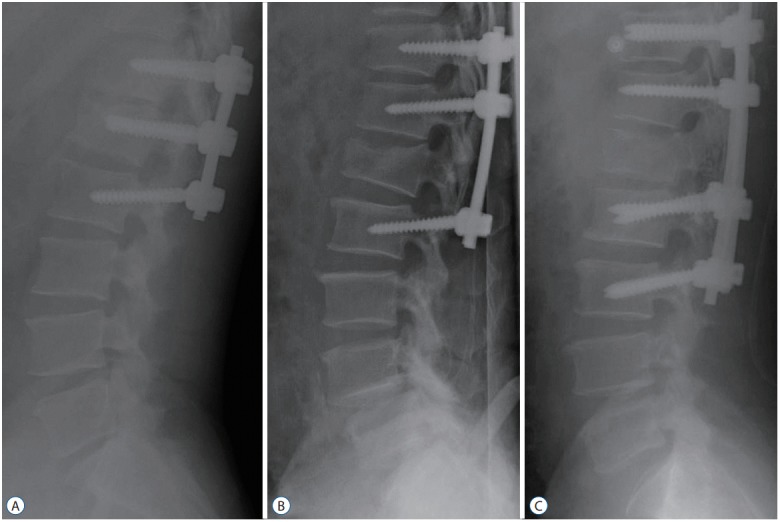
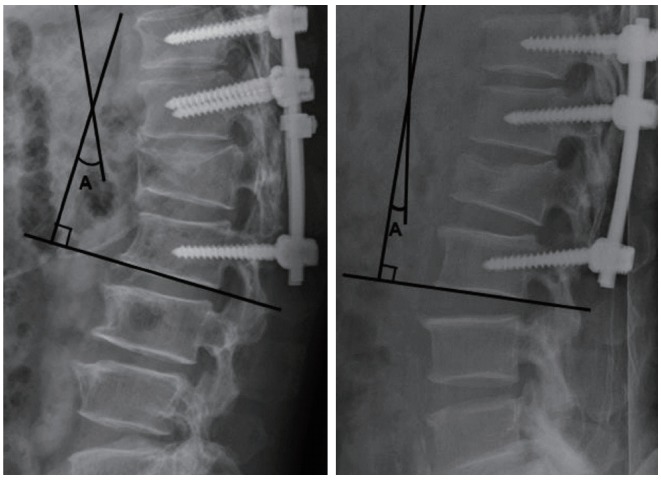
Methods: This study was conducted in a single institution from January 2007 to December 2013. A total of 98 patients with unstable thoracolumbar spine fracture were included. In these patients, fixation was done through transpedicular screws with rods by three surgical patterns. We reviewed digital radiographs and analyzed the images preoperatively and postoperatively during follow-up visits to compare the change of the thoracolumbar Cobb angle with radiologic parameters and clinical outcomes. The unfavorable radiologic group was defined as the patients who were measured as having greater than 20 degrees of thoracolumbar Cobb angle on the last follow-up, or who underwent kyphotic progression of thoracolumbar Cobb angle greater than 10 degrees from the immediate postoperative state to final follow-up, or who had overt instrument failure with/without additional surgery. We assessed the risk factors that affected the unfavorable radiologic outcomes.
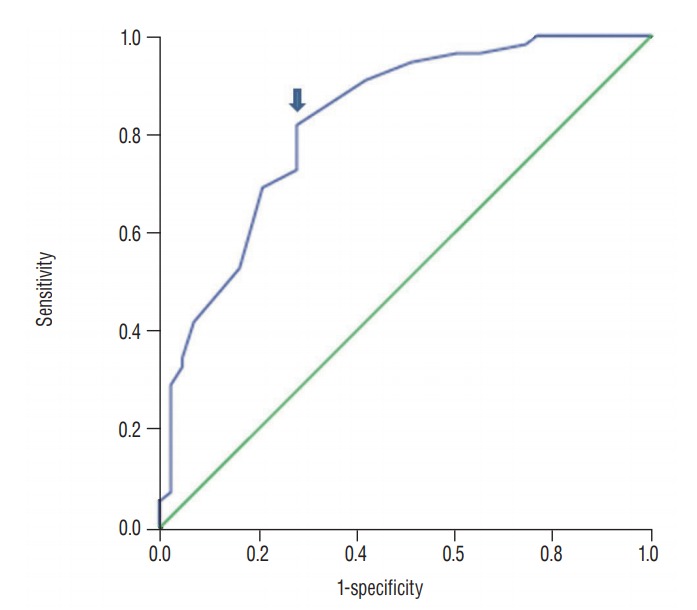
Results: We had 43 patients with unfavorable radiologic outcomes, including 35 abnormal thoracolumbar alignments and 14 instrumental failures with/without additional surgery. The multivariate logistic regression test showed that immediate postoperative T-L junction Cobb angle less than 10.5 degrees was a statistically significant risk factor, as well as the presence of osteoporosis (p=0.017 and 0.049, respectively).
Conclusion: Insufficient correction of thoracolumbar kyphosis was considered to be a major factor of an unfavorable radiological outcome. The spinal surgeon should consider that having a T-L junction Cobb angle larger than 10.5 degrees immediately after surgery could result in an unfavorable radiological outcome, which is related to a poor clinical outcome.
Keywords: Spinal injuries ∙ Thoracic vertebrae ∙ Kyphosis ∙ Risk factors.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Complications and Unfavorable Clinical Outcomes in Obese and Overweight Patients Treated for Adult Lumbar or Thoracolumbar Scoliosis With Combined Anterior/Posterior Surgery.J Spinal Disord Tech. 2015 Jul;28(6):E368-76. doi: 10.1097/BSD.0b013e3182999526. J Spinal Disord Tech. 2015. PMID: 23698107
-
Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedicle-screw instrumentation and fusion.Spine (Phila Pa 1976). 2008 Feb 15;33(4):E100-8. doi: 10.1097/BRS.0b013e3181646b07. Spine (Phila Pa 1976). 2008. PMID: 18277858
-
[Clinical features and strategies for treatment of spinal fracture complicating ankylosing spondylitis].Zhonghua Yi Xue Za Zhi. 2007 Nov 6;87(41):2893-8. Zhonghua Yi Xue Za Zhi. 2007. PMID: 18261302 Chinese.
-
Modified pedicle subtraction osteotomies (mPSO) for thoracolumbar post-tubercular kyphosis in pediatric patients: retrospective clinical cases and review of the literature.Childs Nerv Syst. 2015 Aug;31(8):1347-54. doi: 10.1007/s00381-015-2738-y. Epub 2015 May 8. Childs Nerv Syst. 2015. PMID: 25953095 Review.
-
Management of burst fractures in the thoracolumbar spine.J Orthop. 2016 Jun 28;13(4):278-81. doi: 10.1016/j.jor.2016.06.007. eCollection 2016 Dec. J Orthop. 2016. PMID: 27408503 Free PMC article. Review.
Cited by
-
Characteristics and mechanical mechanisms of intervertebral disc degeneration in old thoracolumbar fractures with kyphosis: clinical observations and finite element analyses.BMC Musculoskelet Disord. 2024 Dec 19;25(1):1040. doi: 10.1186/s12891-024-08157-8. BMC Musculoskelet Disord. 2024. PMID: 39702090 Free PMC article.
-
Clinical and Radiological Factors Affecting Thoracolumbar Fractures Outcome: WFNS Spine Committee Recommendations.Neurospine. 2021 Dec;18(4):693-703. doi: 10.14245/ns.2142518.259. Epub 2021 Dec 31. Neurospine. 2021. PMID: 35000322 Free PMC article.
-
Radiographic Outcomes of Thoracolumbar AOSpine A3 and A4 Fractures Treated With External Bracing.Cureus. 2022 Feb 22;14(2):e22490. doi: 10.7759/cureus.22490. eCollection 2022 Feb. Cureus. 2022. PMID: 35371752 Free PMC article.
-
Radiographic Outcomes of Conservative and Operative Treatment in Isolated L1 Fractures.Medicina (Kaunas). 2023 Apr 1;59(4):695. doi: 10.3390/medicina59040695. Medicina (Kaunas). 2023. PMID: 37109653 Free PMC article.
-
Classification and Radiological Diagnosis of Thoracolumbar Spine Fractures: WFNS Spine Committee Recommendations.Neurospine. 2021 Dec;18(4):656-666. doi: 10.14245/ns.2142650.325. Epub 2021 Dec 31. Neurospine. 2021. PMID: 35000319 Free PMC article.
References
-
- Akbarnia BA, Crandall DG, Burkus K, Matthews T. Use of long rods and a short arthrodesis for burst fractures of the thoracolumbar spine. a long-term follow-up study. J Bone Joint Surg Am. 1994;76:1629–1635. - PubMed
-
- Alanay A, Acaroglu E, Yazici M, Oznur A, Surat A. Short-segment pedicle instrumentation of thoracolumbar burst fractures: does transpedicular intracorporeal grafting prevent early failure? Spine (Phila Pa 1976) 2001;26:213–217. - PubMed
-
- Albayrak A, Balioglu MB, Misir A, Kargin D, Tacal MT, Atici Y, et al. Preoperative and postoperative photographs and surgical outcomes of patients with kyphosis. Spine (Phila Pa 1976) 2016;41:E1185–E1190. - PubMed
-
- Been HD, Bouma GJ. Comparison of two types of surgery for thoracolumbar burst fractures: combined anterior and posterior stabilisation vs. posterior instrumentation only. Acta Neurochir (Wien) 1999;141:349–357. - PubMed
-
- Briggs AM, van Dieën JH, Wrigley TV, Greig AM, Phillips B, Lo SK, et al. Thoracic kyphosis affects spinal loads and trunk muscle force. Phys Ther. 2007;87:595–607. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
