

Biochemical and inflammatory modifications after switching to dual antiretroviral therapy in HIV-infected patients in Italy: a multicenter retrospective cohort study from 2007 to 2015
- PMID: 29940869
- PMCID: PMC6020212
- DOI: 10.1186/s12879-018-3198-2
Biochemical and inflammatory modifications after switching to dual antiretroviral therapy in HIV-infected patients in Italy: a multicenter retrospective cohort study from 2007 to 2015
Abstract
Background: Triple-drug regimens are the gold standard for HIV therapy. Nucleos(t)ide reverse transcriptase inhibitors (NRTIs) reducing regimens are used to decrease drugs toxicity, exposure and costs. Aim of our study was to evaluate trends of biochemical and inflammatory indices in patients switching to dual therapy (DT).
Methods: We included patients that a) switched to a DT from 2007 to 2015 from a tenofovir/abacavir-based triple regimen b) previously maintained a triple and c) subsequently a dual regimen for 12 months with virological suppression. We retrieved data measured at 5 points (at the switch, 6 and 12 months before and after switch). We used platelet-to-lymphocyte ratio (PLR), neutrophil-to-lymphocyte ratio (NLR) and CD4/CD8 ratio as inflammatory indices. We assessed temporal trends of viro-immunological, biochemical and inflammatory parameters.
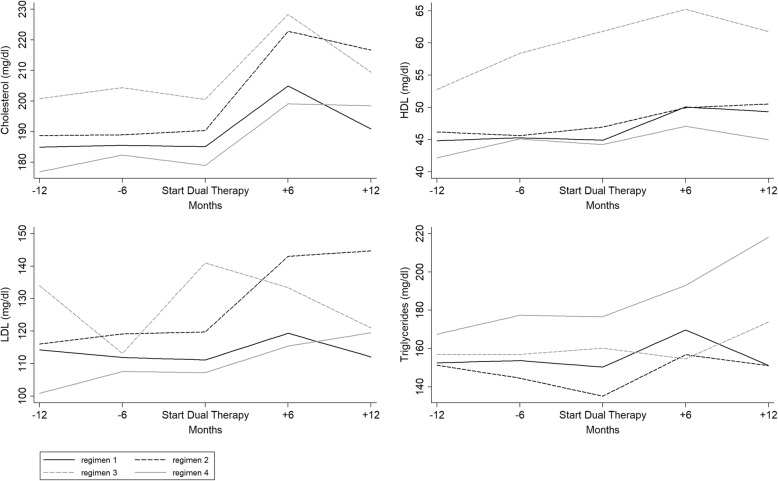
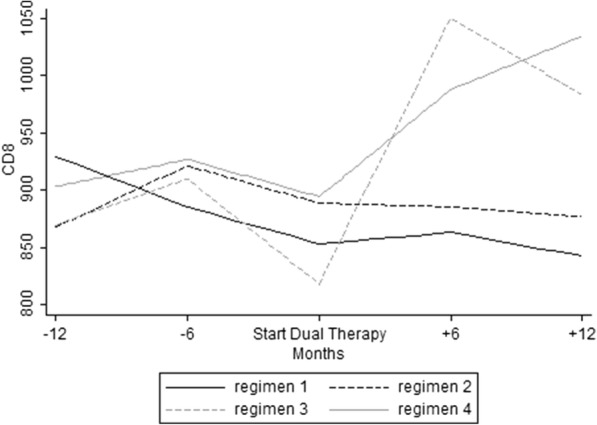
Results: Overall, 364 and 65 patients switched from a tenofovir- and an abacavir-triple regimen, respectively. In the tenofovir-reducing group, creatinine clearance and lipids raised after the switch. There was a significant increase in both CD4+ cells and CD4/CD8. CD8+ cells rose after the switch, while opposite trend was found for PLR. In the abacavir-reducing group total lipids showed a decrease during the first 6 months after the switch and then stabilized. An increase of CD4+ and a decrease of CD8+ cells was observed during the study period, although not statistically significant. While CD4/CD8 remained stable after simplification, PLR decreased significantly after 6 months, then returning to baseline. CD8+ cells increased in the tenofovir-reducing group despite a viro-immunological response. Intriguingly, PLR decreased, maintaining this trend for 12 and 6 months after tenofovir and abacavir interruption respectively.
Conclusions: Increased PLR has been linked to hypercholesterolemia and metabolic-syndrome, while high CD8+ cells count to increased risk of non-AIDS-related events regardless of CD4 T-cell recovery and to virological failure. Whether these findings may have clinical implications, and which role DT plays on the immune system and on inflammation should be further investigated.
Keywords: Antiretroviral therapy; Dual-therapy; HIV; Inflammation; Switch.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Ethic Committee of the Azienda Ospedaliera Spedali Civili of Brescia on the 4th of August, 2009, reference number 708. Written informed consent was obtained by all patients enrolled.
Consent for publication
Not applicable.
Competing interests
EQR received travel grants from Bristol-Myers Squibb, Gilead, Bristol-Myers Squibb, Viiv and Janssen-Cilag; moreover received speaker’s honoraria from Gilead and MSD during the conduct of the study. PM received travel grants from Viiv and Gilead. ER declared no competing interests.
II declared no competing interests. BA reported grants from Bristol-Myers Squibb and Gilead, non-financial support from Bristol-Myers Squibb, Viiv and Janssen-Cilag during the conduct of the study. LF declared no competing interests. SA received travel grants from Bristol-Myers Squibb, Gilead, Bristol-Myers Squibb, Viiv and Janssen-Cilag; moreover received speaker’s honoraria from Bristol-Myers Squibb, Gilead, Bristol-Myers Squibb, Viiv and Janssen-Cilag during the conduct of the study and is currently acting as an Associate Editor for BMC Infectious Diseases. MF declared no competing interests. FC declared no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Montaner JSG, Reiss P, Cooper D, Vella S, Harris M, Conway B, Wainberg MA, Smith D, Robinson P, Hall D, Myers M, Lange JMA, For the INCAS Study Group A randomized, double-blind trial comparing combinations of Nevirapine, Didanosine, and zidovudine for HIV-infected PatientsThe INCAS trial. JAMA. 1998;279(12):930–937. doi: 10.1001/jama.279.12.930. - DOI - PubMed
-
- European AIDS Clinical Society Guidelines 2017. Version 8.2. Available: http://www.eacsociety.org/files/guidelines_8.2-english.pdf. Last accessed: 18 Aug 2017.
-
- World Health Organization Consolidated Guidelines on the use of antiretroviral drugs for treating and preventing of HIV infection. Recomendations for a public approach. 2nd edition, 2016. Available: http://apps.who.int/iris/bitstream/10665/208825/1/9789241549684_eng.pdf Last accessed: 18 Aug 2017.
-
- Società Italiana di Malattie Infettive e Tropicali (SIMIT). Linee guida italiane sull'utilizzo dei farmaci anti-retrovirali e sulla gestione diagnostico-clinica delle persone coinfezione da HIV. Available: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2545_allegato.pdf. Last accessed: 18 Aug 2017.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
