

Hematuria as a risk factor for progression of chronic kidney disease and death: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study
- PMID: 29940877
- PMCID: PMC6020240
- DOI: 10.1186/s12882-018-0951-0
Hematuria as a risk factor for progression of chronic kidney disease and death: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study
Abstract
Background: Hematuria is associated with chronic kidney disease (CKD), but has rarely been examined as a risk factor for CKD progression. We explored whether individuals with hematuria had worse outcomes compared to those without hematuria in the CRIC Study.
Methods: Participants were a racially and ethnically diverse group of adults (21 to 74 years), with moderate CKD. Presence of hematuria (positive dipstick) from a single urine sample was the primary predictor. Outcomes included a 50% or greater reduction in eGFR from baseline, ESRD, and death, over a median follow-up of 7.3 years, analyzed using Cox Proportional Hazards models. Net reclassification indices (NRI) and C statistics were calculated to evaluate their predictive performance.
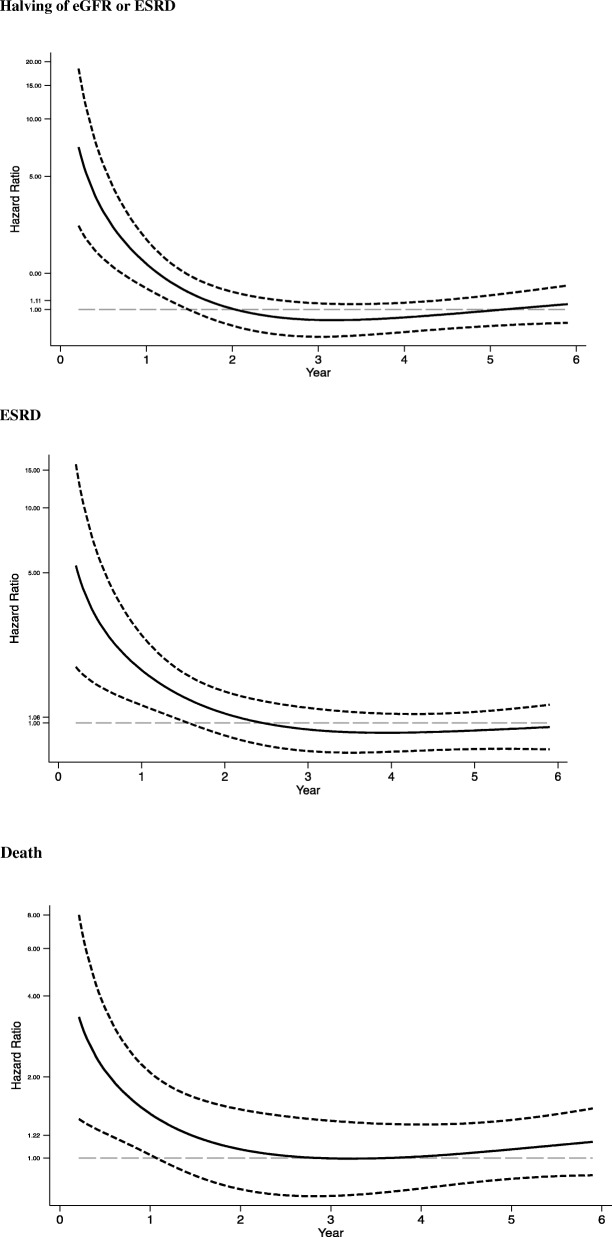
Results: Hematuria was observed in 1145 (29%) of a total of 3272 participants at baseline. Individuals with hematuria were more likely to be Hispanic (22% vs. 9.5%, respectively), have diabetes (56% vs. 48%), lower mean eGFR (40.2 vs. 45.3 ml/min/1.73 m2), and higher levels of urinary albumin > 1.0 g/day (36% vs. 10%). In multivariable-adjusted analysis, individuals with hematuria had a greater risk for all outcomes during the first 2 years of follow-up: Halving of eGFR or ESRD (HR Year 1: 1.68, Year 2: 1.36), ESRD (Year 1: 1.71, Year 2: 1.39) and death (Year 1:1.92, Year 2: 1.77), and these associations were attenuated, thereafter. Based on NRIs and C-statistics, no clear improvement in the ability to improve prediction of study outcomes was observed when hematuria was included in multivariable models.
Conclusion: In a large adult cohort with CKD, hematuria was associated with a significantly higher risk of CKD progression and death in the first 2 years of follow-up but did not improve risk prediction.
Keywords: CKD; CKD progression; ESRD; Epidemiology; Hematuria; Mortality; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
All participants provided written informed consent. The study protocol was approved by the Institutional Review Board of the University of Pennsylvania (protocol number 707819), Johns Hopkins Institutional Review Board (protocol number NA_00044034), University of Maryland Institutional Review Board (protocol number HCR-HP-00041233-9), University Hospitals Institutional Review Board (protocol number 02–03-04), MetroHealth System Institutional Review Board (protocol number IRB03–00052), Cleveland Clinic Institutional Review Board (protocol number 5969), University of Michigan Institutional Review Board (protocol number HUM00073515), Wayne State Institutional Review Board (protocol number 071803MP2F), University of Illinois at Chicago Institutional Review Board (protocol number 2003–0149), Tulane University Institutional Review Board (protocol number 140987–49), Kaiser Permanente Northern California Institutional Review Board (protocol number CN-01AGo-02-H).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Davis R, Jones JS, Barocas DA, et al. Diagnosis, evaluation and follow-up of asymptomatic microhematuria (AMH) in adults: AUA guideline. JURO. 2012;188:2473–2481. - PubMed
-
- Heyman SN, Brezis M. Acute renal failure in glomerular bleeding: a puzzling phenomenon. Nephrol Dial Transplant. 1995;10(5):591–593. - PubMed
-
- Fogazzi GB, Imbasciati E, Moroni G, Scalia A, Mihatsch MJ, Ponticelli C. Reversible acute renal failure from gross haematuria due to glomerulonephritis: not only in IgA nephropathy and not associated with intratubular obstruction. Nephrol Dial Transplant. 1995;10(5):624–629. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR002003/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1TR000433/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
