

Selection of essential medicines for the prevention and treatment of cardiovascular diseases in low and middle income countries
- PMID: 29940880
- PMCID: PMC6019804
- DOI: 10.1186/s12872-018-0858-5
Selection of essential medicines for the prevention and treatment of cardiovascular diseases in low and middle income countries
Abstract
Background: The incidence and mortality of cardiovascular diseases (CVDs) in low and middle income countries (LMICs) have been increasing, while access to CVDs medicines is suboptimal. We assessed selection of essential medicines for the prevention and treatment of CVDs on national essential medicines lists (NEMLs) of LMICs and potential determinants for selection.
Methods: Only operational NEMLs were considered eligible for this study. A selection of medicines listed under "cardiovascular medicines" or "blood products and plasma substitutes" in the NEMLs were included if they were present on international guidelines for the prevention and treatment of CVDs (hyperlipidemia, hypertension, platelet inhibition, ischemic stroke, stable ischemic heart disease, acute coronary syndromes, heart failure, atrial fibrillation, peripheral arterial disease and acute limb ischemia). The number and diversity of essential medicines selected for CVDs were studied. Moreover, determinants of selection of essential medicines for CVDs at a national level were explored. Data analysis was done using univariate linear regression and non-parametric tests.
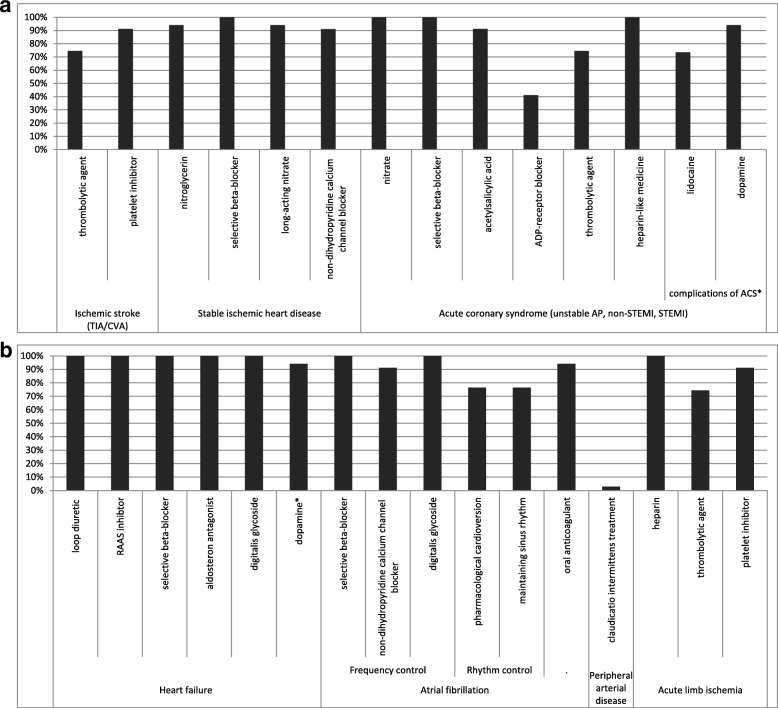
Results: All medicine groups listed by the international guidelines were selected by the majority of the 34 countries studied with the exception of adenosine diphosphate receptor inhibitors which appeared on less than half of the NEMLs studied (41% of countries). The total number of essential medicines for the prevention and treatment of cardiovascular diseases (median 24 (range 16-50)) differed significantly across income levels (median range: 19.5-25, p = 0.014) and across regions (median range: 20-32, p = 0.049). When recommendations of the international guidelines were considered, over 75% of the NEMLs contained essential medicines for the majority of CVDs.
Conclusion: The main medicine classes for the management of CVDs were represented on NEMLs. Consequently, for the majority of CVDs, evidence-based guideline-recommended treatment is possible as far as selection of essential medicines is concerned. Selection will therefore not be the limiting step in access to medicines for cardiovascular diseases.
Keywords: Access to medicines; Cardiovascular diseases; Essential medicines lists; Low and middle income countries.
Conflict of interest statement
Ethics approval and consent to participate
All data were publicly available data at a country level, and therefore no ethical approval was required.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Associations between essential medicines and health outcomes for cardiovascular disease.BMC Cardiovasc Disord. 2021 Mar 25;21(1):151. doi: 10.1186/s12872-021-01955-1. BMC Cardiovasc Disord. 2021. PMID: 33765933 Free PMC article.
-
Access to Cardiovascular Disease and Hypertension Medicines in Developing Countries: An Analysis of Essential Medicine Lists, Price, Availability, and Affordability.J Am Heart Assoc. 2020 May 5;9(9):e015302. doi: 10.1161/JAHA.119.015302. Epub 2020 Apr 25. J Am Heart Assoc. 2020. PMID: 32338557 Free PMC article.
-
Cardiovascular disease essential medicines listing by countries: changes over time and association with health outcomes.BMC Cardiovasc Disord. 2025 Jan 27;25(1):50. doi: 10.1186/s12872-024-04411-y. BMC Cardiovasc Disord. 2025. PMID: 39865241 Free PMC article.
-
Access to Medications for Cardiovascular Diseases in Low- and Middle-Income Countries.Circulation. 2016 May 24;133(21):2076-85. doi: 10.1161/CIRCULATIONAHA.115.008722. Circulation. 2016. PMID: 27217433 Free PMC article. Review.
-
Essential medicines availability is still suboptimal in many countries: a scoping review.J Clin Epidemiol. 2018 Jun;98:41-52. doi: 10.1016/j.jclinepi.2018.02.006. Epub 2018 Feb 13. J Clin Epidemiol. 2018. PMID: 29452222
Cited by
-
β-blockers and metabolic modulation: unraveling the complex interplay with glucose metabolism, inflammation and oxidative stress.Front Pharmacol. 2024 Dec 20;15:1489657. doi: 10.3389/fphar.2024.1489657. eCollection 2024. Front Pharmacol. 2024. PMID: 39759452 Free PMC article. Review.
-
Association between renal function and platelet reactivity during aspirin therapy in elderly patients with atherosclerotic cardiovascular disease.BMC Geriatr. 2021 Jan 22;21(1):75. doi: 10.1186/s12877-021-02018-y. BMC Geriatr. 2021. PMID: 33482738 Free PMC article.
-
Associations between essential medicines and health outcomes for cardiovascular disease.BMC Cardiovasc Disord. 2021 Mar 25;21(1):151. doi: 10.1186/s12872-021-01955-1. BMC Cardiovasc Disord. 2021. PMID: 33765933 Free PMC article.
-
Medical Tourism for Cancer Treatment: Trends, Trajectories, and Perspectives From African Countries.JCO Glob Oncol. 2024 Oct;10:e2400131. doi: 10.1200/GO.24.00131. Epub 2024 Oct 24. JCO Glob Oncol. 2024. PMID: 39447099 Free PMC article.
-
Essential tuberculosis medicines and health outcomes in countries with a national essential medicines list.J Clin Tuberc Other Mycobact Dis. 2022 Feb 23;27:100305. doi: 10.1016/j.jctube.2022.100305. eCollection 2022 May. J Clin Tuberc Other Mycobact Dis. 2022. PMID: 35308809 Free PMC article.
References
-
- Mendis S, Puska P, Norrving B. Global atlas on cardiovascular disease Prevention and Control. In: Mendis S, editor. World Health Organization. 1. Geneva: World Health Organization; 2011. pp. 2–14.
-
- Bovet P, Paccaud F. Cardiovascular disease and the changing face of global public Health : a focus on low and middle income countries. Public Health Rev. 2011;33(2):397–415. doi: 10.1007/BF03391643. - DOI
-
- Mendis S, Alwan A. A prioritized research agenda for prevention and control of noncommunicable diseases. 1. Geneva: World Health Organization; 2011.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
