

Development of practice and consensus-based strategies including a treat-to-target approach for the management of moderate and severe juvenile dermatomyositis in Germany and Austria
- PMID: 29940960
- PMCID: PMC6019723
- DOI: 10.1186/s12969-018-0257-6
Development of practice and consensus-based strategies including a treat-to-target approach for the management of moderate and severe juvenile dermatomyositis in Germany and Austria
Abstract
Background: Juvenile dermatomyositis (JDM) is the most common inflammatory myopathy in childhood and a major cause of morbidity among children with pediatric rheumatic diseases. The management of JDM is very heterogeneous. The JDM working group of the Society for Pediatric Rheumatology (GKJR) aims to define consensus- and practice-based strategies in order to harmonize diagnosis, treatment and monitoring of JDM.
Methods: The JDM working group was established in 2015 consisting of 23 pediatric rheumatologists, pediatric neurologists and dermatologists with expertise in the management of JDM. Current practice patterns of management in JDM had previously been identified via an online survey among pediatric rheumatologists and neurologists. Using a consensus process consisting of online surveys and a face-to-face consensus conference statements were defined regarding the diagnosis, treatment and monitoring of JDM. During the conference consensus was achieved via nominal group technique. Voting took place using an electronic audience response system, and at least 80% consensus was required for individual statements.
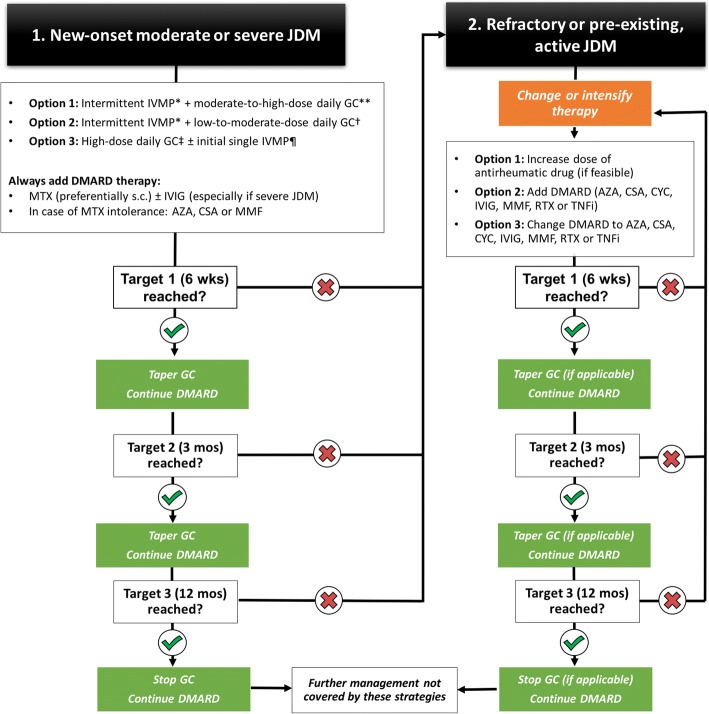
Results: Overall 10 individual statements were developed, finally reaching a consensus of 92 to 100% regarding (1) establishing a diagnosis, (2) case definitions for the application of the strategies (moderate and severe JDM), (3) initial diagnostic testing, (4) monitoring and documentation, (5) treatment targets within the context of a treat-to-target strategy, (6) supportive therapies, (7) explicit definition of a treat-to-target strategy, (8) various glucocorticoid regimens, including intermittent intravenous methylprednisolone pulse and high-dose oral glucocorticoid therapies with tapering, (9) initial glucocorticoid-sparing therapy and (10) management of refractory disease.
Conclusion: Using a consensus process among JDM experts, statements regarding the management of JDM were defined. These statements and the strategies aid in the management of patients with moderate and severe JDM.
Keywords: Antirheumatic agents; Child; Comparative effectiveness research; Consensus; Dermatomyositis; Diagnosis.
Conflict of interest statement
Ethics approval and consent to participate
The national pediatric rheumatology database was approved by the ethics committee of the Charité in Berlin.
Consent for publication
Not applicable.
Competing interests
Dr. Hinze has received consulting fees, speaking fees, and/or honoraria from Novartis (less than $10,000 each). Dr. Oommen reports no potential competing interests. Dr. Dressler has received consulting fees, speaking fees, and/or honoraria from Novartis and Pfizer (less than $10,000 each). Dr. Weller-Heinemann has received honoraria from Abbvie, Novartis and Pfizer (less than $10,000 each). Dr. Lainka has received consulting fees, speaking fees, and/or honoraria from Novartis (less than $10,000 each) and research support from Sobi. Dr. Brunner has received consulting fees, speaking fees, and/or honoraria from Abbvie, MSD, Novartis, Pfizer and Roche (less than $10,000 each). Dr. Föll is a board member of the Society for Pediatric Rheumatoloy and has received honoraria from Novartis, Pfizer, Roche-Chugai and Sobi (less than $10,000 each) and research support from Novartis and Pfizer. Dr. Neudorf has received consulting fees, speaking fees, and/or honoraria from Chugai and Philips (less than $10,000 each), and research support from Novartis. Dr. Schwarz reports no potential competing interests. Dr. Schara is president of the Gesellschaft für Neuropädiatrie (GNP; Society for Pediatric Neurology in Germany) and has received consulting fees, speaking fees, and/or honoraria from PTC Therapeutics, Deutsche Myasthenie Gesellschaft (German Myasthenia Society) and benni &co (a non-profit organization benifitting patients with muscular dystrophy). Dr. Haas is the president of the Society for Pediatric Rheumatology has received research support from Novartis and Pfizer.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Stringer E, Bohnsack J, Bowyer SL, Griffin TA, Huber AM, Lang B, Lindsley CB, Ota S, Pilkington C, Reed AM, et al. Treatment approaches to juvenile dermatomyositis (JDM) across North America: the childhood arthritis and rheumatology research alliance (CARRA) JDM treatment survey. J Rheumatol. 2010;37(9):1953–1961. doi: 10.3899/jrheum.090953. - DOI - PubMed
-
- Oddis CV, Reed AM, Aggarwal R, Rider LG, Ascherman DP, Levesque MC, Barohn RJ, Feldman BM, Harris-Love MO, Koontz DC, et al. Rituximab in the treatment of refractory adult and juvenile dermatomyositis and adult polymyositis: a randomized, placebo-phase trial. Arthritis Rheum. 2013;65(2):314–324. doi: 10.1002/art.37754. - DOI - PMC - PubMed
-
- Ruperto N, Pistorio A, Oliveira S, Zulian F, Cuttica R, Ravelli A, Fischbach M, Magnusson B, Sterba G, Avcin T, et al. Prednisone versus prednisone plus ciclosporin versus prednisone plus methotrexate in new-onset juvenile dermatomyositis: a randomised trial. Lancet. 2016;387(10019):671–678. doi: 10.1016/S0140-6736(15)01021-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
