

Assessing health status over time: impact of recall period and anchor question on the minimal clinically important difference of copd health status tools
- PMID: 29940980
- PMCID: PMC6019834
- DOI: 10.1186/s12955-018-0950-7
Assessing health status over time: impact of recall period and anchor question on the minimal clinically important difference of copd health status tools
Abstract
Background: The Minimal Clinically Important Difference (MCID) assesses what change on a measurement tool can be considered minimal clinically relevant. Although the recall period can influence questionnaire scores, it is unclear if it influences the MCID. This study is the first to examine longitudinally the impact of the recall period of an anchor question and its design on the MCID of COPD health status tools using the COPD Assessment Test (CAT), Clinical COPD Questionnaire (CCQ) and the St. George's Respiratory Questionnaire (SGRQ).
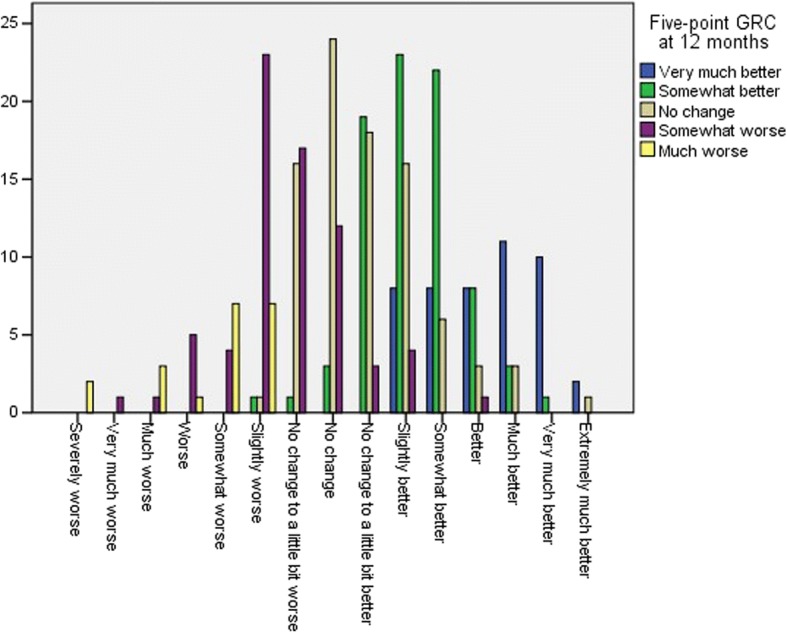
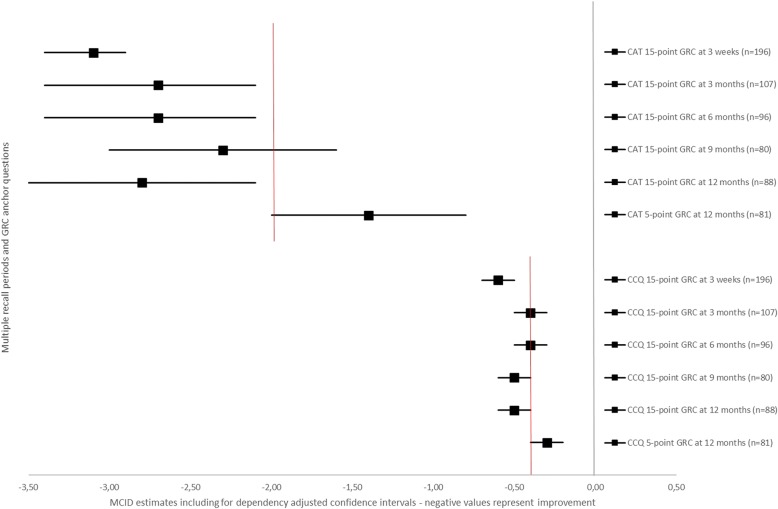
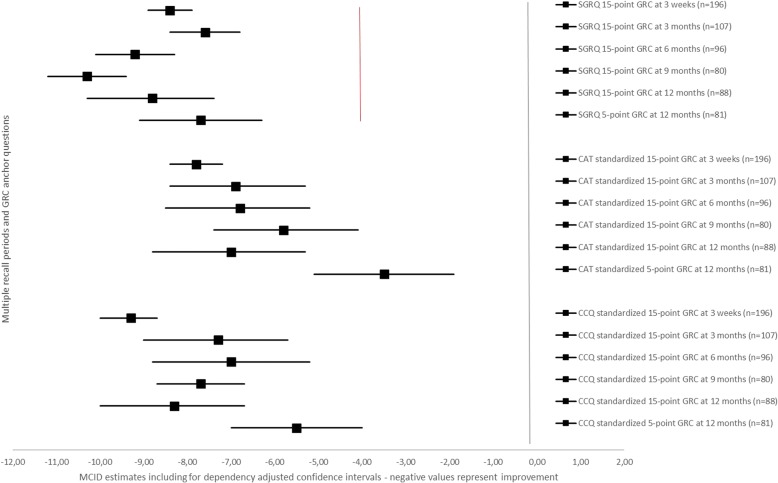
Methods: Moderate to very severe COPD patients without respiratory co-morbidities were recruited during 3-week Pulmonary Rehabilitation (PR). CAT, CCQ and SGRQ were completed at baseline, discharge, 3, 6, 9 and 12 months. A 15-point Global Rating of Change scale (GRC) was completed at each follow-up. A five-point GRC was used as second anchor at 12 months. Mean change scores of a subset of patients indicating a minimal improvement on each of the anchor questions were considered the MCID. The MCID estimates over different time periods were compared with one another by evaluating the degree of overlap of Confidence Intervals (CI) adjusted for dependency.
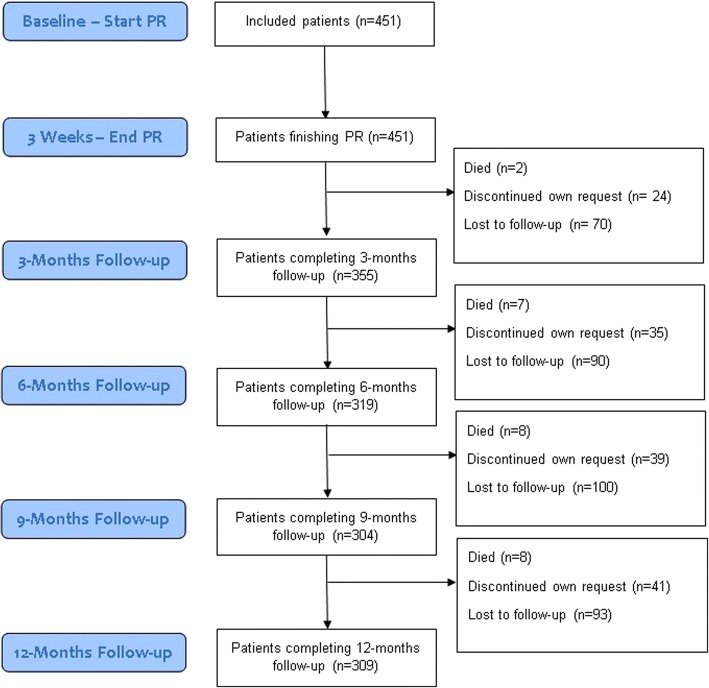
Results: In total 451 patients were included (57.9 ± 6.6 years, 65% male, 50/39/11% GOLD II/III/IV), of which 309 completed follow-up. Baseline health status scores were 20.2 ± 7.3 (CAT), 2.9 ± 1.2 (CCQ) and 50.7 ± 17.3 (SGRQ). MCID estimates for improvement ranged - 3.1 to - 1.4 for CAT, - 0.6 to - 0.3 for CCQ, and - 10.3 to - 7.6 for SGRQ. Absolute higher - though not significant - MCIDs were observed for CAT and CCQ directly after PR. Significantly absolute lower MCID estimates were observed for CAT (difference - 1.4: CI -2.3 to - 0.5) and CCQ (difference - 0.2: CI -0.3 to -0.1) using a five-point GRC.
Conclusions: The recall period of a 15-point anchor question seemed to have limited impact on the MCID for improvement of CAT, CCQ and SGRQ during PR; although a 3-week MCID estimate directly after PR might lead to absolute higher values. However, the design of the anchor question was likely to influence the MCID of CAT and CCQ.
Trial registration: RIMTCORE trial # DRKS00004609 and #12107 (Ethik-Kommission der Bayerischen Landesärztekammer).
Keywords: COPD assessment test (CAT); Chronic obstructive pulmonary disease (COPD); Clinical COPD questionnaire (CCQ); Clinically relevant change; Global rating of change scale; Health status; Minimal clinically important difference; Pulmonary rehabilitation; Recall period; St. George’s respiratory questionnaire (SGRQ).
Conflict of interest statement
Ethics approval and consent to participate
This study is a secondary analysis of a subsample from the Routine Inspiratory Muscle Training within COPD Rehabilitation (RIMTCORE) real-life randomized controlled trial (#DRKS00004609) in the Klinik Bad Reichenhall, Center for Rehabilitation, Pulmonology and Orthopaedics in Germany. All patients signed informed consent upon participation. The RIMTCORE trial was approved by the Ethik-Kommission der Bayerischen Landesärztekammer (#12107) and registered in the German Clinical Trial Register.
Consent of publication
All authors participated in various steps in the study, edited the manuscript and gave their approval for submission.
Competing interests
H.J. Alma, C. de Jong, D. Jelusic, M. Wittmann, M. Schuler, B.J. Kollen and R. Sanderman have nothing to disclose. J.W.H. Kocks reports personal fees from Novartis; research grants and personal fees from Boehringer Ingelheim; research grants and personal fees from GSK; research grants from Stichting Zorgdraad; personal fees from IPCRG; personal fees from Springer Media; and travel arrangements from Chiesi BV, GlaxoSmithKline BV, and IPCRG, all outside the submitted work. K. Schultz received lecture fees from Boehringer, AstraZeneca, Berlin Chemie, Novartis, Chiesi, Mundipharma, Takeda, GSK and MSD, all outside the submitted work. T. van der Molen reports personal reimbursements from GSK, TEVA, Astra Zeneca, Boehringer Ingelheim and study grants from Astra Zeneca and GSK. After this study was terminated, he became employee of GSK. None of these stated conflicts of interest are linked to the current manuscript. T. van der Molen developed the CCQ and holds the copyright.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Health status instruments for patients with COPD in pulmonary rehabilitation: defining a minimal clinically important difference.NPJ Prim Care Respir Med. 2016 Sep 1;26:16041. doi: 10.1038/npjpcrm.2016.41. NPJ Prim Care Respir Med. 2016. PMID: 27597571 Free PMC article.
-
Thresholds for clinically important deterioration versus improvement in COPD health status: results from a randomised controlled trial in pulmonary rehabilitation and an observational study during routine clinical practice.BMJ Open. 2019 Jun 28;9(6):e025776. doi: 10.1136/bmjopen-2018-025776. BMJ Open. 2019. PMID: 31256021 Free PMC article. Clinical Trial.
-
Responsiveness and MCID Estimates for CAT, CCQ, and HADS in Patients With COPD Undergoing Pulmonary Rehabilitation: A Prospective Analysis.J Am Med Dir Assoc. 2017 Jan;18(1):53-58. doi: 10.1016/j.jamda.2016.08.002. Epub 2016 Sep 10. J Am Med Dir Assoc. 2017. PMID: 27624705
-
Clinically relevant differences in COPD health status: systematic review and triangulation.Eur Respir J. 2018 Sep 6;52(3):1800412. doi: 10.1183/13993003.00412-2018. Print 2018 Sep. Eur Respir J. 2018. PMID: 30139774
-
Efficacy of pulmonary rehabilitation in improving the quality of life for patients with chronic obstructive pulmonary disease: Evidence based on nineteen randomized controlled trials.Int J Surg. 2020 Jan;73:78-86. doi: 10.1016/j.ijsu.2019.11.033. Epub 2019 Dec 13. Int J Surg. 2020. PMID: 31843677
Cited by
-
Validity of EQ-5D utility index and minimal clinically important difference estimation among patients with chronic obstructive pulmonary disease.BMC Pulm Med. 2020 Mar 23;20(1):73. doi: 10.1186/s12890-020-1116-z. BMC Pulm Med. 2020. PMID: 32293387 Free PMC article.
-
Commentary: "Healthcare Professionals' Preferred Efficacy Endpoints and Minimal Clinically Important Differences in the Assessment of New Medicines for Chronic Obstructive Pulmonary Disease" by Dankers M et al. in Frontiers in Pharmacology 2020; 10: 1519.Front Pharmacol. 2020 Jun 2;11:827. doi: 10.3389/fphar.2020.00827. eCollection 2020. Front Pharmacol. 2020. PMID: 32581793 Free PMC article. No abstract available.
-
An investigation of methods to improve recall for the patient-reported outcome measurement in COPD patients: a pilot randomised control trial and feasibility study protocol.Pilot Feasibility Stud. 2019 Jul 18;5:92. doi: 10.1186/s40814-019-0475-9. eCollection 2019. Pilot Feasibility Stud. 2019. PMID: 31360536 Free PMC article.
-
Brazilian version of the Clinical COPD Questionnaire, administered by interview: reliability and validity measurement properties.J Bras Pneumol. 2021 May 31;47(3):e20200371. doi: 10.36416/1806-3756/e20200371. eCollection 2021. J Bras Pneumol. 2021. PMID: 34076173 Free PMC article.
-
Predictors of Quality-of-Life Improvement at Different Minimum Clinically Important Difference Values in Patients with Chronic Obstructive Pulmonary Disease after Climatic Rehabilitation Treatment.Life (Basel). 2023 Aug 17;13(8):1763. doi: 10.3390/life13081763. Life (Basel). 2023. PMID: 37629620 Free PMC article.
References
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
