

Clinical evaluation of intensity-modulated radiotherapy for locally advanced pancreatic cancer
- PMID: 29940984
- PMCID: PMC6019294
- DOI: 10.1186/s13014-018-1063-5
Clinical evaluation of intensity-modulated radiotherapy for locally advanced pancreatic cancer
Abstract
Background: The purpose was to retrospectively evaluate the effect of intensity-modulated radiotherapy (IMRT) on gastrointestinal (GI) toxicities and outcomes compared to three-dimensional conformal radiotherapy (3DCRT) for locally advanced pancreatic cancer (LAPC).
Methods: We included 107 consecutive patients who underwent CRT for LAPC from September 2001 to March 2015; 80 patients underwent 3DCRT and 27 patients underwent IMRT. They were compared for GI toxicities, locoregional progression free survival (LRPFS), distant metastasis free survival (DMS), and overall survival (OS).
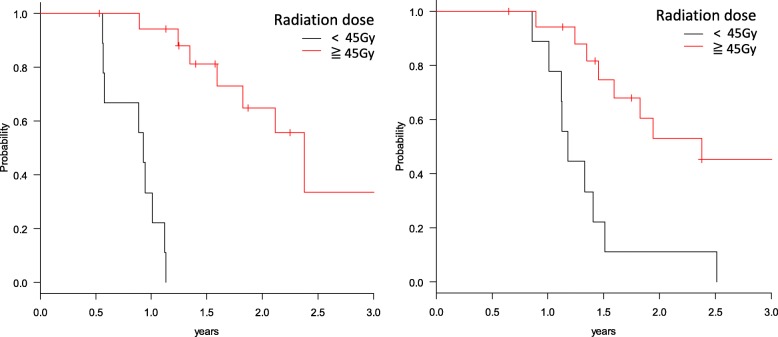
Results: Median radiation dose and fractions for 3DCRT and IMRT were 54 Gy/30 fr. and 48 Gy/15 fr. The regimens of CRT consisted of weekly gemcitabine 250 mg/m2 (for 3DCRT) or 1000 mg/m2 (for IMRT). Acute GI toxicity ≥grade 2 occurred in 32 patients (40%) treated with 3DCRT compared with five patients (19%) treated with IMRT. Late GI toxicity of grade 3 occurred in 10 patients (12%) treated with 3DCRT and one patient (4%) treated with IMRT. Patients who underwent IMRT had superior 1-year LRPFS (73.1% vs. 63.2%, p = 0.035) and 1-year OS (92.3% vs. 68.2%, p = 0.037) as compared with those treated with 3DCRT. Multivariate analysis showed that in IMRT patients, higher dose (≥45 Gy) was an independent factor for better LRPFS and OS.
Conclusions: LAPC patients treated with hypofractionated full-dose gemcitabine IMRT had improved OS and LRPFS without increased GI toxicities when compared to those of patients treated with conventionally fractionated low dose gemcitabine 3DCRT. In IMRT patients, higher dose was an independent favorable prognostic factor for better LRPFS and OS, which suggests that dose escalation with IMRT for LAPC is a promising strategy.
Keywords: Chemoradiotherapy; Intensity-modulated radiotherapy; Locally advanced pancreatic cancer; Treatment result.
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained and chart reviews were performed after approval by the ethics committee of Kyoto University Hospital.
Consent for publication
Not Applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Iacobuzio-Donahue CA, Fu B, Yachida S, Luo M, Abe H, Henderson CM, et al. DPC4 gene status of the primary carcinoma correlates with patterns of failure in patients with pancreatic cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2009;27:1806–1813. doi: 10.1200/JCO.2008.17.7188. - DOI - PMC - PubMed
-
- Klaassen DJ, MacIntyre JM, Catton GE, Engstrom PF, Moertel CG. Treatment of locally unresectable cancer of the stomach and pancreas: a randomized comparison of 5-fluorouracil alone with radiation plus concurrent and maintenance 5-fluorouracil--an eastern cooperative oncology group study. J Clin Oncol : official journal of the American Society of Clinical Oncology. 1985;3:373–378. doi: 10.1200/JCO.1985.3.3.373. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
