

Surgical management of chronic lateral ankle instability: a meta-analysis
- PMID: 29940985
- PMCID: PMC6019311
- DOI: 10.1186/s13018-018-0870-6
Surgical management of chronic lateral ankle instability: a meta-analysis
Abstract
Background: A key point to surgical treatment of chronic lateral ankle instability is choosing a suitable surgical procedure. The purpose of this meta-analysis was to compare different surgical techniques for management of chronic lateral ankle instability.
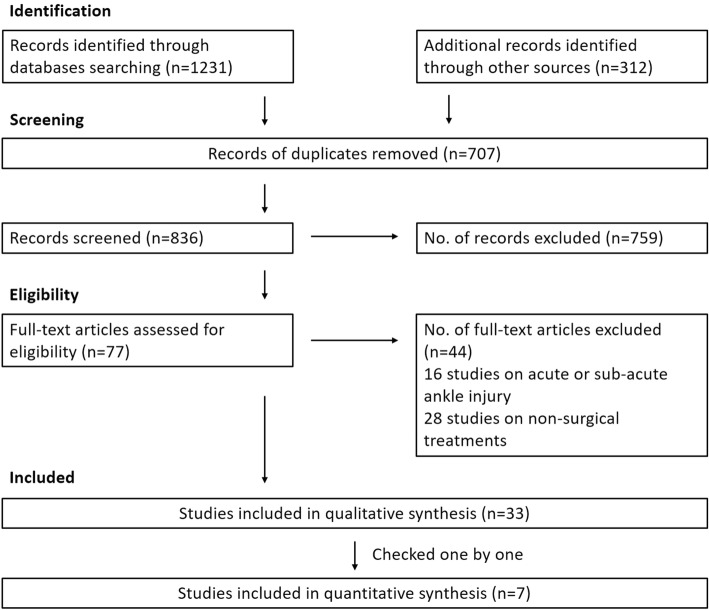
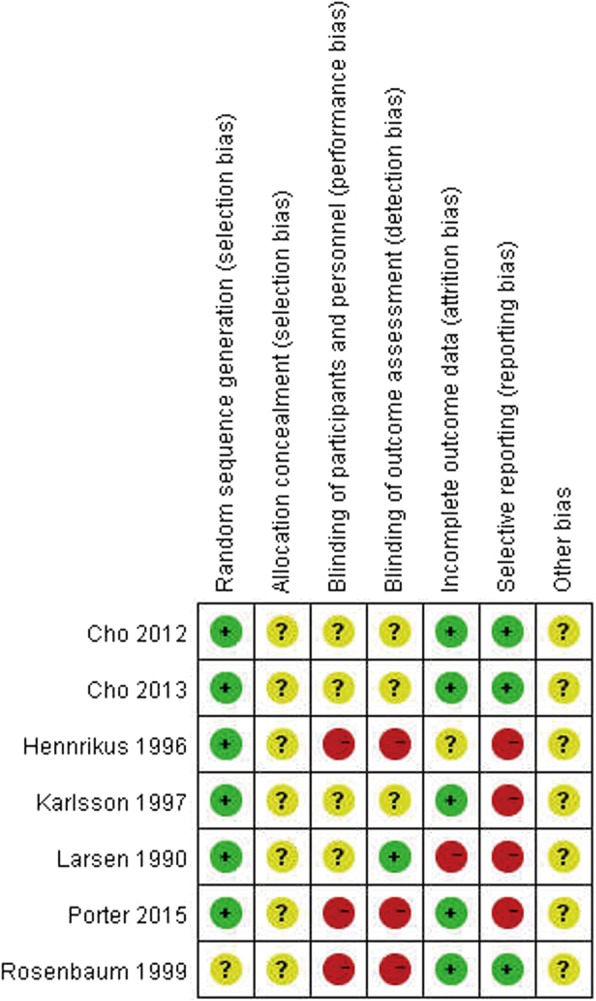
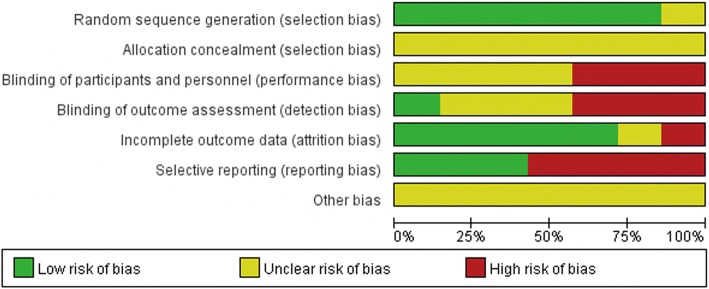
Methods: We searched the Cochrane Library, MEDLINE, and EMBASE. All identified randomized and quasi-randomized controlled trials of operative treatment for chronic lateral ankle instability were included. Two review authors independently extracted data from each study and assessed risk of bias. Where appropriate, results of comparable studies were pooled.
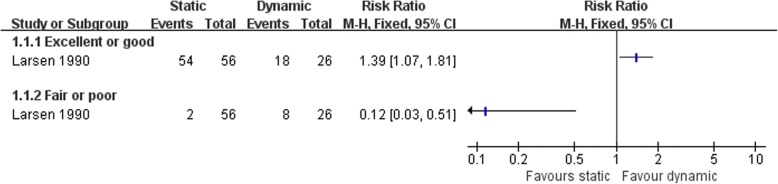
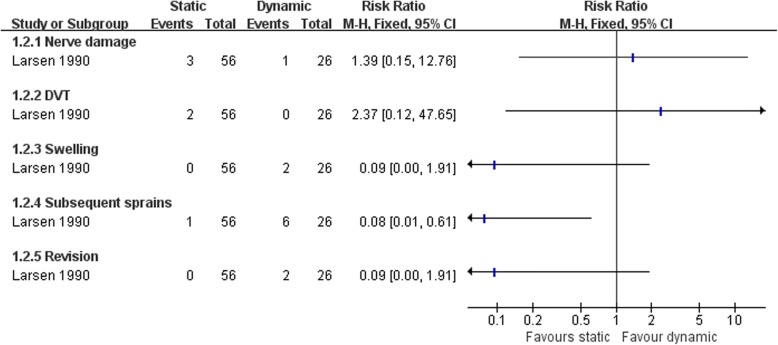
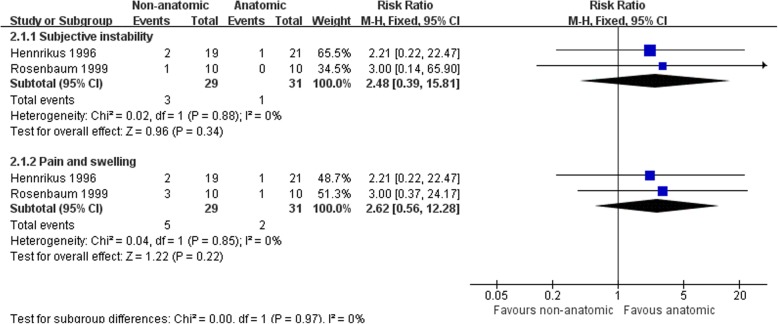
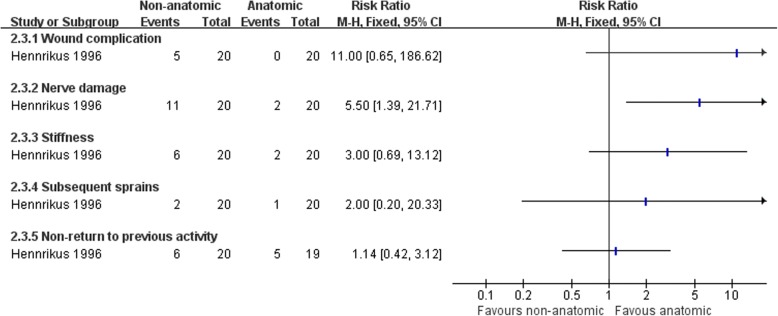
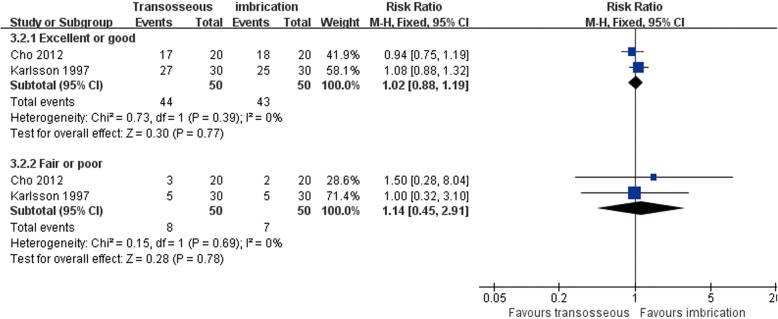
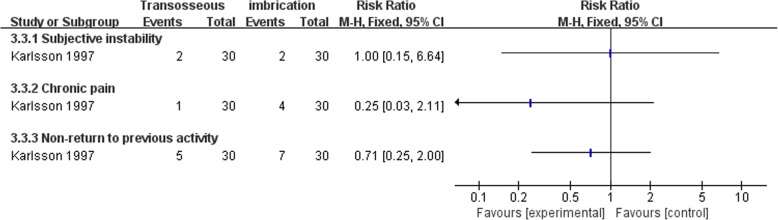
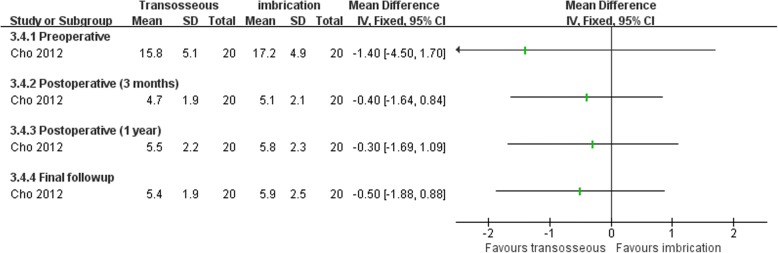
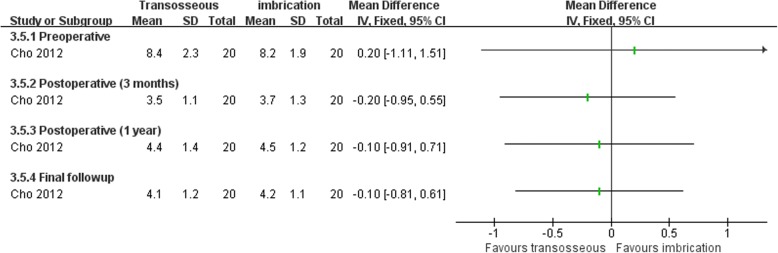
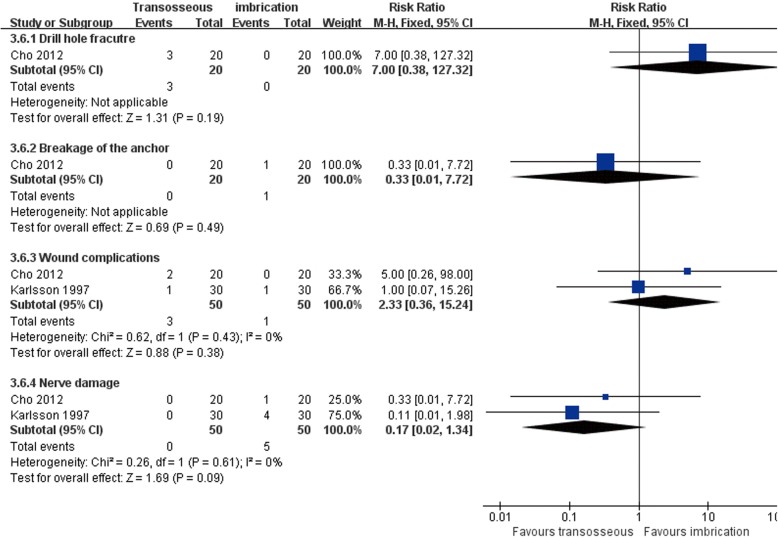
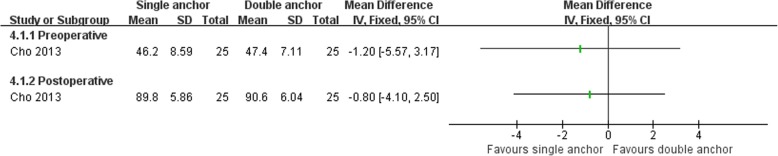
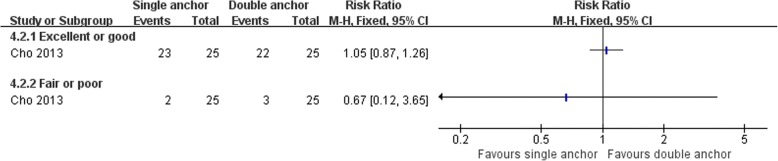
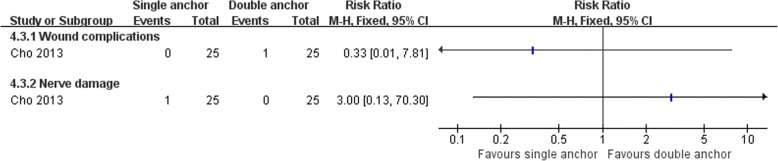
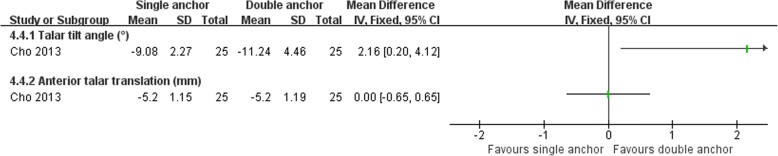
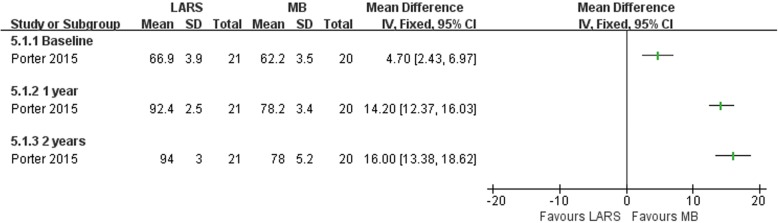
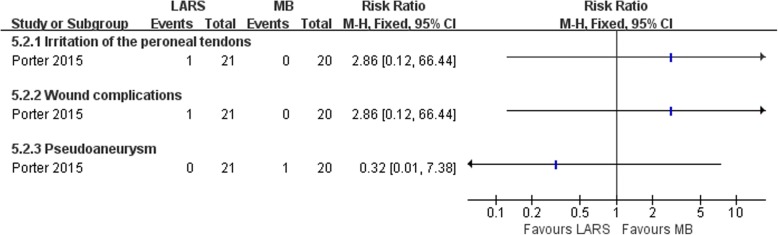
Results: Seven randomized controlled trials were included for analysis. They fell in five clearly distinct groups. One study comparing two different kinds of non-anatomic reconstruction procedures (dynamic and static tenodesis) found two clinical outcomes favoring static tenodesis: better clinical satisfaction and fewer subsequent sprains. Two studies compared non-anatomic reconstruction versus anatomic repairment. In one study, nerve damage was more frequent in non-anatomic reconstruction group; the other one reported that radiological measurement of ankle laxity showed that non-anatomic reconstruction provided higher reduction of talar tilt angle. Two studies comparing two anatomic repairment surgical techniques (transosseous suture versus imbrication) showed no significant difference in any clinical outcome at the follow-up except operation time. One study compared two different anatomic repairment techniques. They found that the double anchor technique was superior with respect to the reduction of talar tilt than single anchor technique. One study compared an anatomic reconstruction procedure with a modified Brostrom technique. Primary reconstruction combined with ligament advanced reinforcement system results in better patient-scored clinical outcome, at 2 years post-surgery, than the modified Brostrom procedure.
Conclusions: There is limited evidence to support any one surgical technique over another surgical technique for chronic lateral ankle instability, but based on the evidence, we could still get some conclusions: (1) There are limitations to the use of dynamic tenodesis, which obtained poor clinical satisfaction and more subsequent sprains. (2) Non-anatomic reconstruction abnormally increased inversion stiffness at the subtalar level as compare with anatomic repairment. (3) Multiple types of modified Brostrom procedures could acquire good clinical results. (4) Anatomic reconstruction is a better procedure for some specific patients.
Keywords: Ankle instability; Ankle sprain; Lateral ligament injury; Meta-analysis; Surgical treatment.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable. All analyses were based on previous published studies; thus, no ethical approval and patient consent are required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Guillo S, Bauer T, Lee JW, Takao M, Kong SW, Stone JW, Mangone PG, Molloy A, Perera A, Pearce CJ, et al. Consensus in chronic ankle instability: aetiology, assessment, surgical indications and place for arthroscopy. Orthop Traumatol Surg Res. 2013;99:S411–S419. doi: 10.1016/j.otsr.2013.10.009. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
