

The evolving epidemiology of Clostridium difficile infection in Canadian hospitals during a postepidemic period (2009-2015)
- PMID: 29941432
- PMCID: PMC6019340
- DOI: 10.1503/cmaj.180013
The evolving epidemiology of Clostridium difficile infection in Canadian hospitals during a postepidemic period (2009-2015)
Abstract
Background: The clinical and molecular epidemiology of health care-associated Clostridium difficile infection in nonepidemic settings across Canada has evolved since the first report of the virulent North American pulsed-field gel electrophoresis type 1 (NAP1) strain more than 15 years ago. The objective of this national, multicentre study was to describe the evolving epidemiology and molecular characteristics of health care-associated C. difficile infection in Canada during a post-NAP1-epidemic period, particularly patient outcomes associated with the NAP1 strain.
Methods: Adult inpatients with C. difficile infection were prospectively identified, using a standard definition, between 2009 and 2015 through the Canadian Nosocomial Infection Surveillance Program (CNISP), a network of 64 acute care hospitals. Patient demographic characteristics, severity of infection and outcomes were reviewed. Molecular testing was performed on isolates, and strain types were analyzed against outcomes and epidemiologic trends.
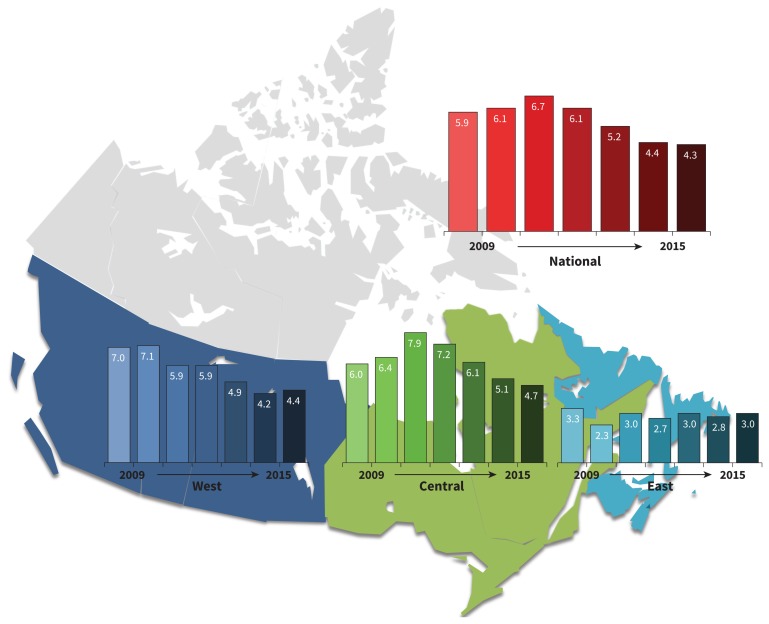
Results: Over a 7-year period, 20 623 adult patients admitted to hospital with health care-associated C. difficile infection were reported to CNISP, and microbiological data were available for 2690 patients. From 2009 to 2015, the national rate of health care-associated C. difficile infection decreased from 5.9 to 4.3 per 10 000 patient-days. NAP1 remained the dominant strain type, but infection with this strain has significantly decreased over time, followed by an increasing trend of infection with NAP4 and NAP11 strains. The NAP1 strain was significantly associated with a higher rate of death attributable to C. difficile infection compared with non-NAP1 strains (odds ratio 1.91, 95% confidence interval [CI] 1.29-2.82). Isolates were universally susceptible to metronidazole; one was nonsusceptible to vancomycin. The proportion of NAP1 strains within individual centres predicted their rates of health care-associated C. difficile infection; for every 10% increase in the proportion of NAP1 strains, the rate of health care-associated C. difficile infection increased by 3.3% (95% CI 1.7%-4.9%).
Interpretation: Rates of health care-associated C. difficile infection have decreased across Canada. In nonepidemic settings, NAP4 has emerged as a common strain type, but NAP1, although decreasing, continues to be the predominant circulating strain and remains significantly associated with higher attributable mortality.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Andrew Simor reports honoraria from Merck Canada. Yves Longtin reports grants from Merck and Becton Dickinson. No other competing interests were declared.
Figures
References
-
- Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol 2010;31:431–55. - PubMed
-
- Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile–associated diarrhea with high morbidity and mortality. N Engl J Med 2005;353:2442–9. - PubMed
-
- Denève C, Janoir C, Poilane I, et al. New trends in Clostridium difficile virulence and pathogenesis. Int J Antimicrob Agents 2009;33(suppl 1):S24–8. - PubMed
-
- Miller M, Gravel D, Mulvey M, et al. Health care-associated Clostridium difficile infection in Canada: patient age and infecting strain type are highly predictive of severe outcome and mortality. Clin Infect Dis 2010;50:194–201. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources