

Causal Inference in Cancer Epidemiology: What Is the Role of Mendelian Randomization?
- PMID: 29941659
- PMCID: PMC6522350
- DOI: 10.1158/1055-9965.EPI-17-1177
Causal Inference in Cancer Epidemiology: What Is the Role of Mendelian Randomization?
Abstract
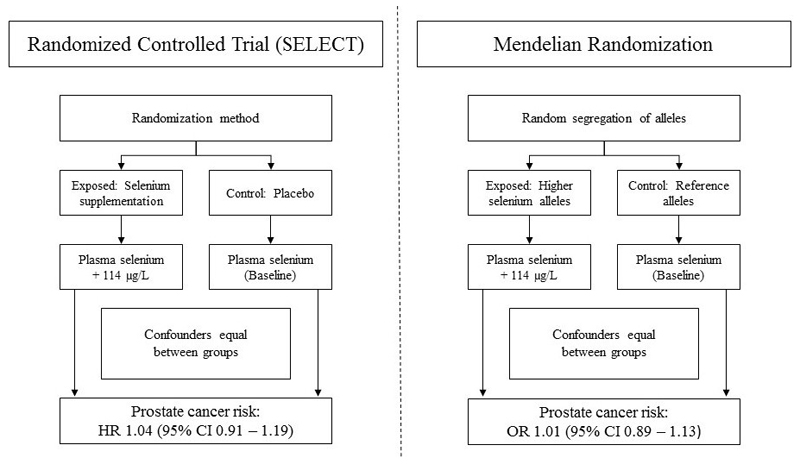
Observational epidemiologic studies are prone to confounding, measurement error, and reverse causation, undermining robust causal inference. Mendelian randomization (MR) uses genetic variants to proxy modifiable exposures to generate more reliable estimates of the causal effects of these exposures on diseases and their outcomes. MR has seen widespread adoption within cardio-metabolic epidemiology, but also holds much promise for identifying possible interventions for cancer prevention and treatment. However, some methodologic challenges in the implementation of MR are particularly pertinent when applying this method to cancer etiology and prognosis, including reverse causation arising from disease latency and selection bias in studies of cancer progression. These issues must be carefully considered to ensure appropriate design, analysis, and interpretation of such studies. In this review, we provide an overview of the key principles and assumptions of MR, focusing on applications of this method to the study of cancer etiology and prognosis. We summarize recent studies in the cancer literature that have adopted a MR framework to highlight strengths of this approach compared with conventional epidemiological studies. Finally, limitations of MR and recent methodologic developments to address them are discussed, along with the translational opportunities they present to inform public health and clinical interventions in cancer. Cancer Epidemiol Biomarkers Prev; 27(9); 995-1010. ©2018 AACR.
©2018 American Association for Cancer Research.
Conflict of interest statement
All authors declare no potential conflicts of interest.
Figures
Similar articles
-
Mendelian randomization: genetic anchors for causal inference in epidemiological studies.Hum Mol Genet. 2014 Sep 15;23(R1):R89-98. doi: 10.1093/hmg/ddu328. Epub 2014 Jul 4. Hum Mol Genet. 2014. PMID: 25064373 Free PMC article. Review.
-
Applying Mendelian randomization to appraise causality in relationships between nutrition and cancer.Cancer Causes Control. 2022 May;33(5):631-652. doi: 10.1007/s10552-022-01562-1. Epub 2022 Mar 11. Cancer Causes Control. 2022. PMID: 35274198 Free PMC article.
-
Causal inference in health and disease: a review of the principles and applications of Mendelian randomization.J Bone Miner Res. 2024 Oct 29;39(11):1539-1552. doi: 10.1093/jbmr/zjae136. J Bone Miner Res. 2024. PMID: 39167758 Free PMC article. Review.
-
Review of Mendelian Randomization Studies on Ovarian Cancer.Front Oncol. 2021 Aug 11;11:681396. doi: 10.3389/fonc.2021.681396. eCollection 2021. Front Oncol. 2021. PMID: 34458137 Free PMC article. Review.
-
A Guide to Understanding Mendelian Randomization Studies.Arthritis Care Res (Hoboken). 2024 Nov;76(11):1451-1460. doi: 10.1002/acr.25400. Epub 2024 Aug 7. Arthritis Care Res (Hoboken). 2024. PMID: 39030941 Free PMC article. Review.
Cited by
-
Genetically proxied therapeutic inhibition of lipid-lowering drug targets and risk of rheumatoid arthritis disease: a Mendelian randomization study.Clin Rheumatol. 2024 Mar;43(3):939-947. doi: 10.1007/s10067-023-06837-9. Epub 2024 Jan 10. Clin Rheumatol. 2024. PMID: 38198113
-
Causal relationship between dietary factors and breast cancer risk: A Mendelian randomization study.Heliyon. 2023 Oct 14;9(10):e20980. doi: 10.1016/j.heliyon.2023.e20980. eCollection 2023 Oct. Heliyon. 2023. PMID: 37867896 Free PMC article.
-
Combining gene expression microarrays and Mendelian randomization: exploring key immune-related genes in multiple sclerosis.Front Neurol. 2024 Nov 27;15:1437778. doi: 10.3389/fneur.2024.1437778. eCollection 2024. Front Neurol. 2024. PMID: 39664749 Free PMC article.
-
Mendelian Randomization Study on hs-CRP and Dyslipidemia in Koreans: Identification of Novel SNP rs76400217.Int J Mol Sci. 2025 Jan 9;26(2):506. doi: 10.3390/ijms26020506. Int J Mol Sci. 2025. PMID: 39859220 Free PMC article.
-
Causal inference in the diagnosis and prognosis of ovarian cancer: current state and future directions.Clin Transl Oncol. 2025 Jun 19. doi: 10.1007/s12094-025-03967-1. Online ahead of print. Clin Transl Oncol. 2025. PMID: 40537725 Review.
References
-
- Taubes G. Epidemiology faces its limits. Science. 1995;269(5221):164–169. - PubMed
-
- Davey Smith G, Ebrahim S. Epidemiology--is it time to call it a day? Int J Epidemiol. 2001;30(1):1–11. - PubMed
-
- Schoenfeld JD, Ioannidis JP. Is everything we eat associated with cancer? A systematic cookbook review. Am J Clin Nutr. 2013;97(1):127–134. - PubMed
-
- Vineis P, Alavanja M, Buffler P, et al. Tobacco and cancer: recent epidemiological evidence. J Natl Cancer Inst. 2004;96(2):99–106. - PubMed
-
- Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45(4):529–538. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
