

Pelvic Exenteration for Recurrent and Persistent Cervical Cancer
- PMID: 29941707
- PMCID: PMC6032675
- DOI: 10.4103/0366-6999.235111
Pelvic Exenteration for Recurrent and Persistent Cervical Cancer
Abstract
Background: Pelvic exenteration (PE) for primary and recurrent cervical cancer has resulted in favorable survival outcomes, but there are controversies about specific prognosis factors, and up to now, there have been no published reports from China. This study aimed to share our experiences of PE, which were performed in a single institution.
Methods: From January 2009 to January 2016, 38 patients with recurrent or persistent cervical cancer were included in the study, and they were followed up until January 2017. Epidemiological and clinicopathological characteristics of patients were compared for survival outcomes in univariate and Cox hazard regression analysis.
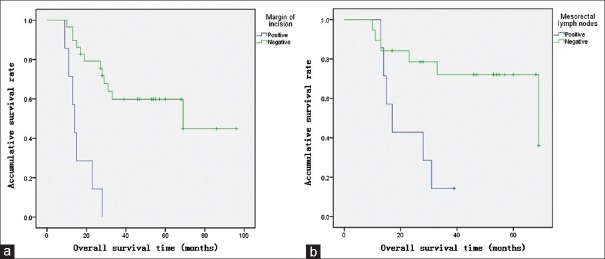
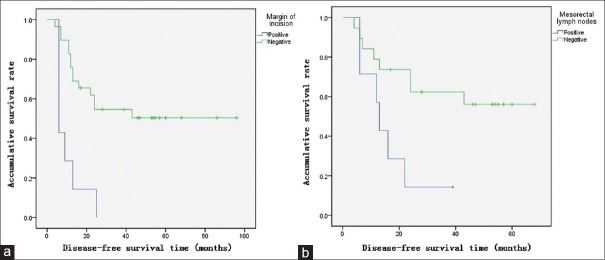
Results: There were thirty-one and seven patients with recurrent and persistent cervical cancer, respectively. The median age of patients was 45 years (range 29-65 years). Total, anterior, and posterior PE consisted of 52.6%, 28.9%, and 18.4% of cases, respectively. Early and late complications occurred in 21 (55.3%) patients and 15 (39.5%) patients, respectively. Two (5.3%) patients died due to complications related to surgeries within 3 months after PE. The median overall survival (OS) and disease-free survival (DFS) were 28.5 months (range 9-96 months) and 23 months (range 4-96 months), respectively, and 5-year OS and DFS were 48% and 40%, respectively. Cox hazard regression analysis showed that, the margin status of the incision and mesorectal lymph node status were independent risk factors for OS and DFS.
Conclusion: In our patients with recurrent and persistent cervical cancer, the practice of PE might achieve favorable survival outcomes.
Trial registration: ClinicalTrials.gov, NCT03291275; https://clinicaltrials.gov/ct2/show/NCT03291275?term=NCT03291275&rank=1.
盆腔廓清术治疗复发性及未控性宫颈癌摘要背景:盆腔廓清术(PE)治疗原发和复发性宫颈癌的生存预后较好,但是有关预后因素仍有很多争议,迄今也没有来自中文的报道。本研究旨在分享我们施行PE的经验,所有手术均在一家医院进行。 方法:从2009年1月到2016年1月,38例复发性或未控性宫颈癌纳入研究,随访至2017年1月。以单因素分析和Cox风险回归模型分析患者流行病学和临床病理特点对生存结局的影响。 结果:复发性和未控性宫颈癌患者分别31例和7例,中位年龄45岁(范围29-65岁)。全盆腔廓清术、前盆腔廓清术和后盆腔廓清术分别占52.6%、28.9%和18.4%。分别有21例(55.3%)和15例(39.5%)患者在术后发生了早期合并症和晚期合并症。两例患者(5.3%)在PE术后3个月内死于合并症。中位总体生存率(OS)和无病生存率(DFS)分别为28.5个月(范围9-96个月)和23个月(范围4-96个月),5年OS率和DFS率分别为48%和40%。Cox风险回归分析显示,切缘状态、直肠系膜淋巴结状态是影响OS和DFS的独立的预后因素。 结论:在我们的研究中,复发和未控性宫颈癌患者在盆腔廓清术后可能有较好的预后结果。 研究注册:ClinicalTrials.gov, NCT03291275; https://clinicaltrials.gov/ct2/show/NCT03291275?term=NCT03291275&rank=1.
Keywords: Cervical Cancer; Pelvic Exenteration; Survival.
Conflict of interest statement
There are no conflicts of interest
Figures
Similar articles
-
Neoadjuvant chemotherapy prior to pelvic exenteration in patients with recurrent cervical cancer: single institution experience.Gynecol Oncol. 2013 Jul;130(1):69-74. doi: 10.1016/j.ygyno.2013.02.038. Epub 2013 Mar 6. Gynecol Oncol. 2013. PMID: 23474343
-
[Outcomes of perisurgery and short-time follow-up of pelvic exenteration for 17 cases with locally recurrent cervical cancer].Zhonghua Fu Chan Ke Za Zhi. 2020 Apr 25;55(4):259-265. doi: 10.3760/cma.j.cn112141-20200119-00049. Zhonghua Fu Chan Ke Za Zhi. 2020. PMID: 32375433 Chinese.
-
Indications for primary and secondary exenterations in patients with cervical cancer.Gynecol Oncol. 2006 Dec;103(3):1023-30. doi: 10.1016/j.ygyno.2006.06.027. Epub 2006 Aug 4. Gynecol Oncol. 2006. PMID: 16890276
-
Laparoscopic pelvic exenteration: a new option in the surgical treatment of locally advanced and recurrent cervical carcinoma.Bratisl Lek Listy. 2008;109(10):467-9. Bratisl Lek Listy. 2008. PMID: 19166135 Review.
-
Pelvic exenteration for carcinoma of the cervix: analysis of 252 cases.J Surg Oncol. 1988 Jun;38(2):121-5. doi: 10.1002/jso.2930380214. J Surg Oncol. 1988. PMID: 3288809 Review.
Cited by
-
Analysis of long-term outcomes in 44 patients following pelvic exenteration due to cervical cancer.World J Surg Oncol. 2020 Sep 2;18(1):234. doi: 10.1186/s12957-020-01997-3. World J Surg Oncol. 2020. PMID: 32878646 Free PMC article.
-
Dosimetry comparison between a 3D printed minimally invasive guidance template and free implantation in the brachytherapy treatment of postoperative recurrent cervical carcinoma.Cancer Manag Res. 2019 May 30;11:5013-5018. doi: 10.2147/CMAR.S195829. eCollection 2019. Cancer Manag Res. 2019. PMID: 31213915 Free PMC article.
-
Re-Irradiation with Intensity-Modulated Radiation Therapy for the Treatment of Recurrent Cervical Cancer in the Pelvis: An Analysis of Outcomes and Toxicity.Medicina (Kaunas). 2023 Jun 17;59(6):1164. doi: 10.3390/medicina59061164. Medicina (Kaunas). 2023. PMID: 37374368 Free PMC article.
-
Salvage Treatment and Outcomes of Locally Advanced Cervical Cancer after Failed Concurrent Chemoradiation with or without Adjuvant Chemotherapy: Post Hoc Data Analysis from the ACTLACC Trial.Asian Pac J Cancer Prev. 2022 Jul 1;23(7):2263-2269. doi: 10.31557/APJCP.2022.23.7.2263. Asian Pac J Cancer Prev. 2022. PMID: 35901330 Free PMC article.
-
Pelvic Exenteration for the Treatment of Locally Advanced Vulvar Cancer in South West Wales.Cancers (Basel). 2022 Mar 31;14(7):1767. doi: 10.3390/cancers14071767. Cancers (Basel). 2022. PMID: 35406539 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. doi: 10.3322/caac.21332. - PubMed
-
- Waggoner SE. Cervical cancer. Lancet. 2003;361:2217–25. doi: 10.1016/s0140-6736(03)13778-6. - PubMed
-
- Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, et al. Bethesda, MD: National Cancer Institute; 1975-2012. [Last accessed on 2015 Apr 01]. SEER Cancer Statistics Review. Available from: http://www.seer.cancer.gov .
-
- Landoni F, Maneo A, Colombo A, Placa F, Milani R, Perego P, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997;350:535–40. doi: 10.1016/s0140-6736(97)02250-2. - PubMed
-
- Rose PG, Bundy BN, Watkins EB, Thigpen JT, Deppe G, Maiman MA, et al. Concurrent cisplatin-based radiotherapy and chemotherapy for locally advanced cervical cancer. N Engl J Med. 1999;340:1144–53. doi: 10.1056/nejm199904153401502. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
