

Polypoidal choroidal vasculopathy: Pearls in diagnosis and management
- PMID: 29941728
- PMCID: PMC6032720
- DOI: 10.4103/ijo.IJO_1136_17
Polypoidal choroidal vasculopathy: Pearls in diagnosis and management
Abstract
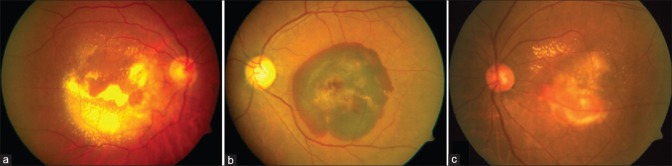
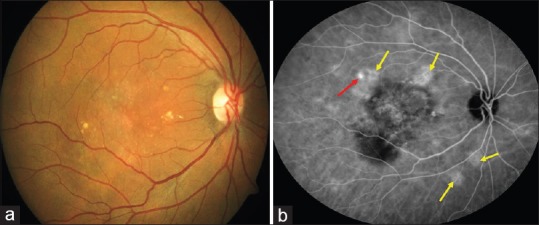
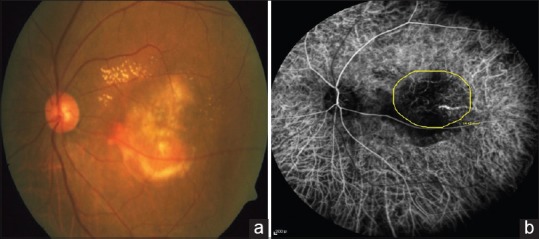
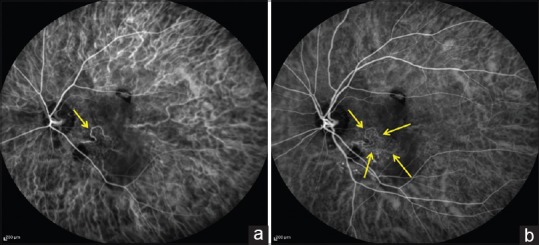
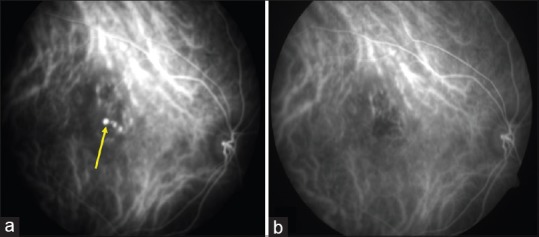
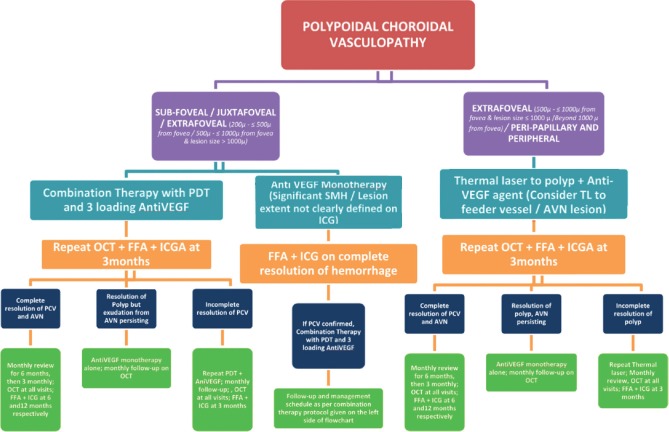
Polypoidal choroidal vasculopathy (PCV) is increasingly recognized as an important cause of exudative maculopathy in Asians as against Wet age-related macular degeneration in Caucasians. A panel of retinal experts methodically evaluated pertinent updated literature on PCV with thorough PubMed/MEDLINE search. Based on this, the panel agreed upon and proposed the current consensus recommendations in the diagnosis (clinical and imaging), management and follow-up schedule of PCV. Diagnosis of PCV should be based on the gold standard indocyanine green angiography which demonstrates early nodular hyperfluorescence signifying the polyp with additional features such as abnormal vascular network (AVN). Optical coherence tomography is an excellent adjuvant for diagnosing PCV, monitoring disease activity, and decision-making regarding the treatment. Current treatment modalities for PCV include photodynamic therapy, anti-vascular endothelial growth factor agents, and thermal laser. Choice of specific treatment modality and prognosis depends on multiple factors such as the location and size of PCV lesion, presence or absence of polyp with residual AVN, amount of submacular hemorrhage, presence or absence of leakage on fundus fluorescein angiography, visual acuity, and so on. Current recommendations would be invaluable for the treating physician in diagnosing PCV and in formulating the best possible individualized treatment strategy for optimal outcomes in PCV management.
Keywords: Abnormal vascular network; indocyanine green angiography; optical coherence tomography; photodynamic therapy; polypoidal choroidal vasculopathy; thermal laser.
Conflict of interest statement
There are no conflicts of interest
Figures



References
-
- Yannuzzi LA. Miami, FL: 1982. Idiopathic polypoidal choroidal vasculopathy. Macula Society Meeting.
-
- Liu Y, Wen F, Huang S, Luo G, Yan H, Sun Z, et al. Subtype lesions of neovascular age-related macular degeneration in chinese patients. Graefes Arch Clin Exp Ophthalmol. 2007;245:1441–5. - PubMed
-
- Maruko I, Iida T, Saito M, Nagayama D, Saito K. Clinical characteristics of exudative age-related macular degeneration in Japanese patients. Am J Ophthalmol. 2007;144:15–22. - PubMed
-
- Chang YC, Wu WC. Polypoidal choroidal vasculopathy in Taiwanese patients. Ophthalmic Surg Lasers Imaging. 2009;40:576–81. - PubMed
-
- Byeon SH, Lee SC, Oh HS, Kim SS, Koh HJ, Kwon OW, et al. Incidence and clinical patterns of polypoidal choroidal vasculopathy in Korean patients. Jpn J Ophthalmol. 2008;52:57–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
