

Novel techniques in scleral buckling
- PMID: 29941729
- PMCID: PMC6032754
- DOI: 10.4103/ijo.IJO_136_18
Novel techniques in scleral buckling
Abstract
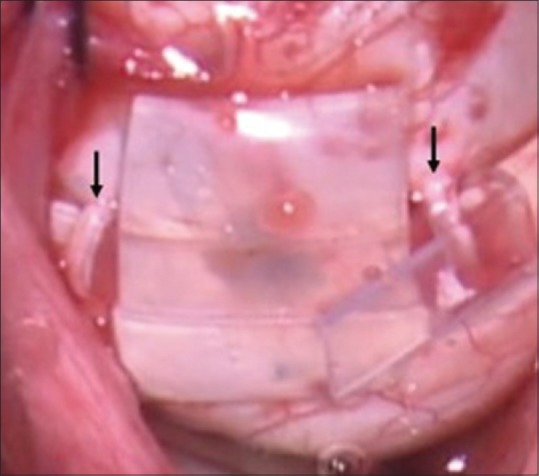
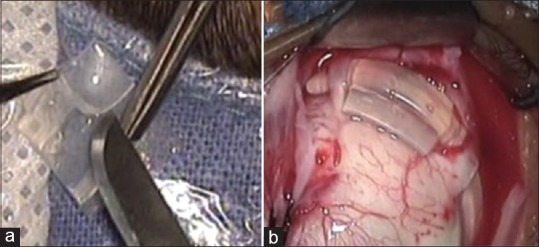
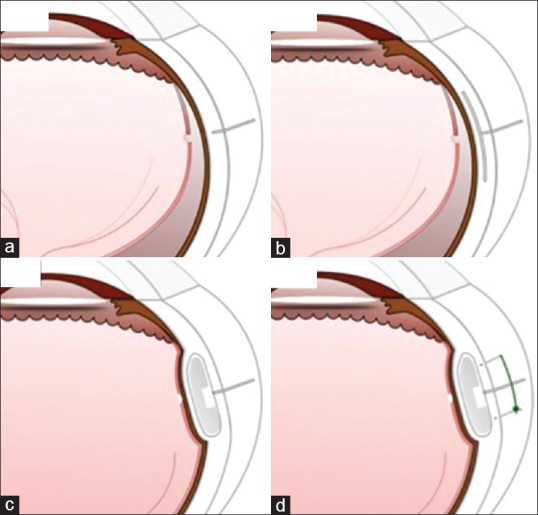
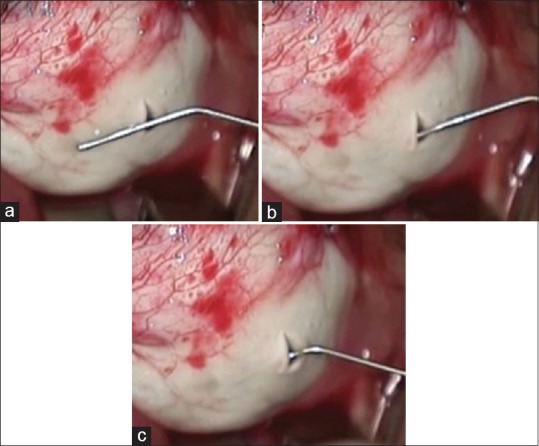
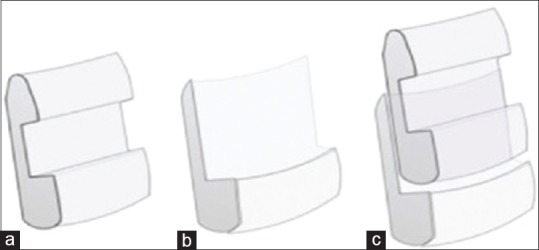
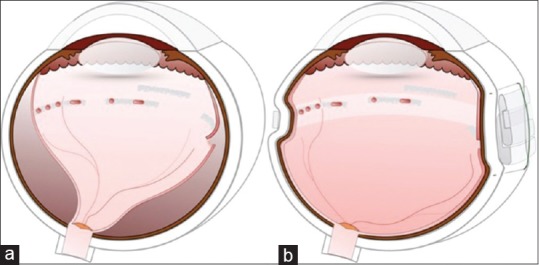
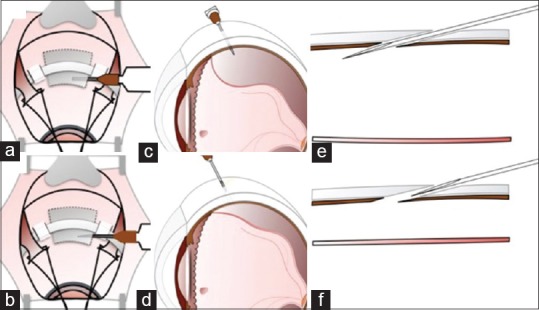
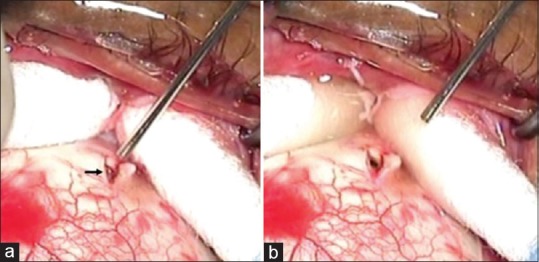
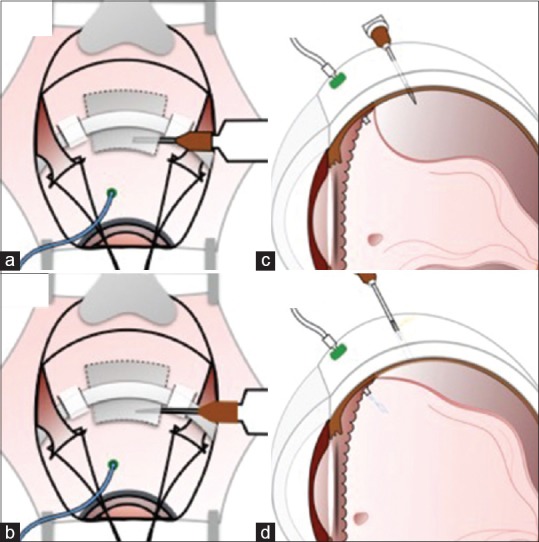
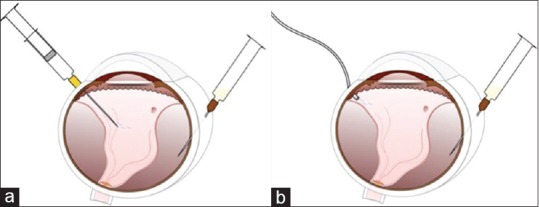
Scleral buckling is a surgical technique that is employed successfully to treat rhegmatogenous retinal detachments (RRD) for more than 60 years. With the introduction of pars plana vitrectomy (PPV), there is a growing trend towards the use of PPV for treatment of retinal detachment. There is a reluctance to perform scleral buckling (SB) in RRD due to the perceived steep learning curve, declining mastery over indirect ophthalmoscopy, and poor ergonomics associated with SB. In this article, we discuss the surgical challenges and tips to overcome these in four headings: localization of the break, retinopexy, SB, and subretinal fluid (SRF) drainage. Localization of the break can be performed by the use of forceps or illuminated scleral depressor. It can be facilitated by prior drainage of SRF in cases with bullous RRD. Chandelier with wide-angle viewing system can be used for easier localization of break and cryopexy. Sutureless buckling and suprachoroidal buckling are easier and faster alternatives to the conventional technique. Reshaping the silicone segment helps in accommodating the wider circumferential band. Modified needle drainage, laser choroidotomy, and infusion-assisted drainage can make SRF drainage easier and safer. The above techniques and other practical tips have been explained in detail with the illustrations to make the process of learning the art of SB easier.
Keywords: Retinal detachment; retinopexy; scleral buckling; subretinal fluid drainage.
Conflict of interest statement
There are no conflicts of interest
Figures








References
-
- Blodi BA, Paluska SA. Cataract after vitrectomy in young patients. Ophthalmology. 1997;104:1092–5. - PubMed
-
- Hotta K, Sugitani A. Refractive changes in silicone oil-filled pseudophakic eyes. Retina. 2005;25:167–70. - PubMed
-
- Stefánsson E, Anderson MM, Jr, Landers MB, 3rd, Tiedeman JS, McCuen BW., 2nd Refractive changes from use of silicone oil in vitreous surgery. Retina. 1988;8:20–3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
