

Molecular phenomics and metagenomics of hepatic steatosis in non-diabetic obese women
- PMID: 29942096
- PMCID: PMC6140997
- DOI: 10.1038/s41591-018-0061-3
Molecular phenomics and metagenomics of hepatic steatosis in non-diabetic obese women
Erratum in
-
Publisher Correction: Molecular phenomics and metagenomics of hepatic steatosis in non-diabetic obese women.Nat Med. 2018 Oct;24(10):1628. doi: 10.1038/s41591-018-0169-5. Nat Med. 2018. PMID: 30093731
Abstract
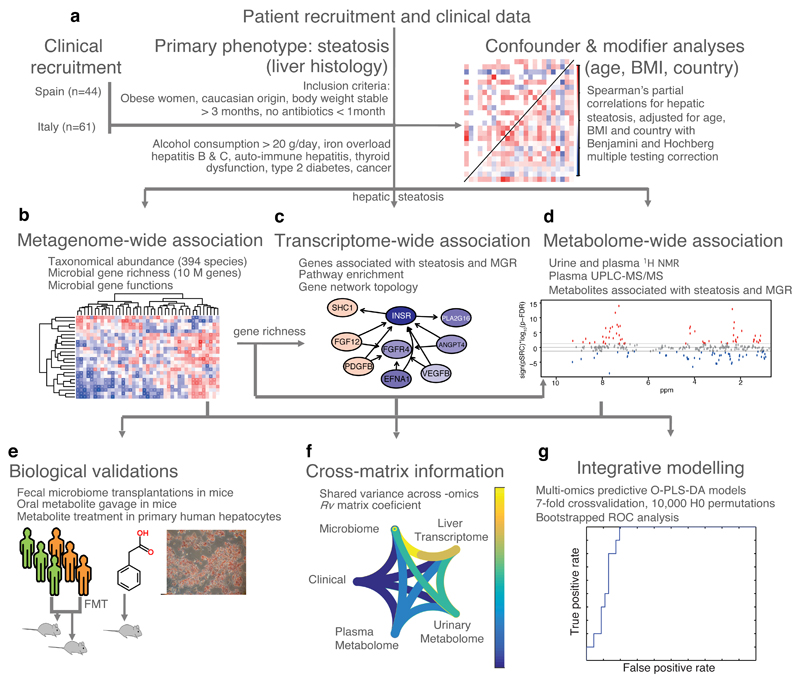
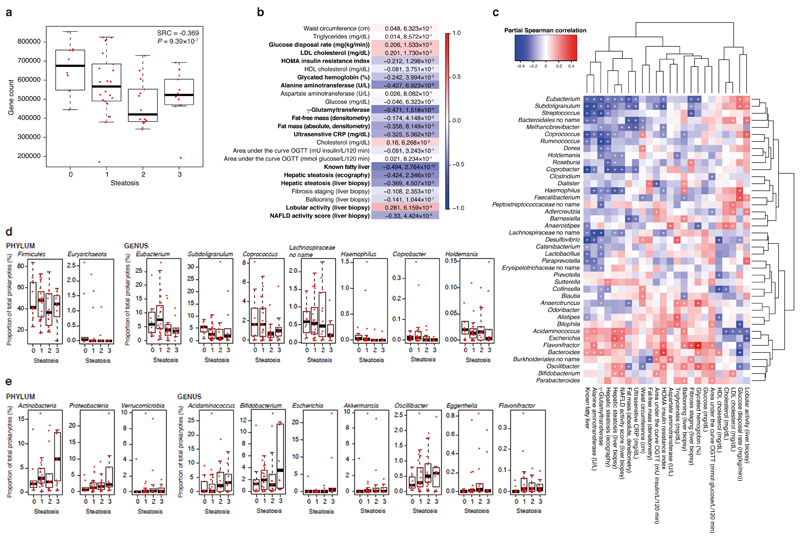
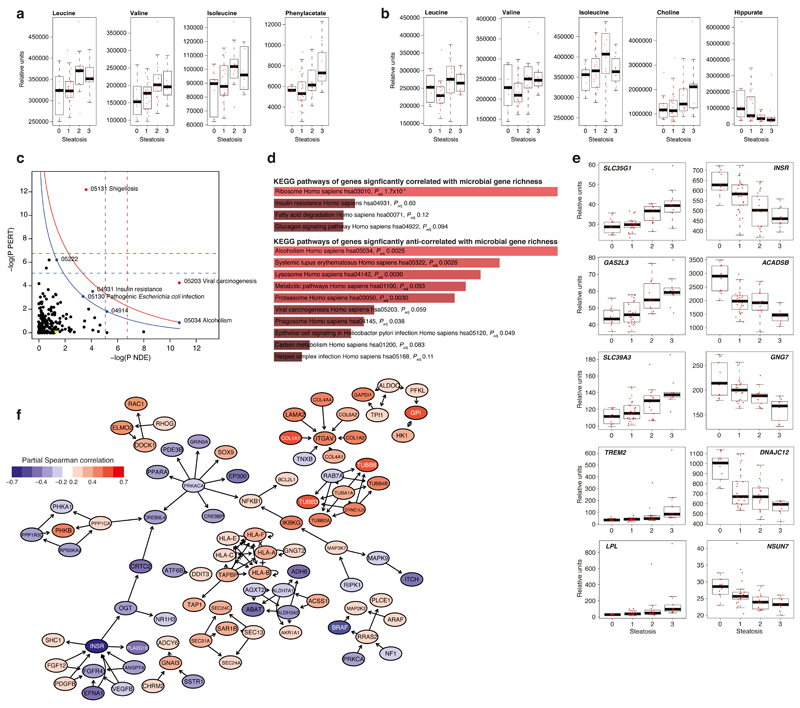
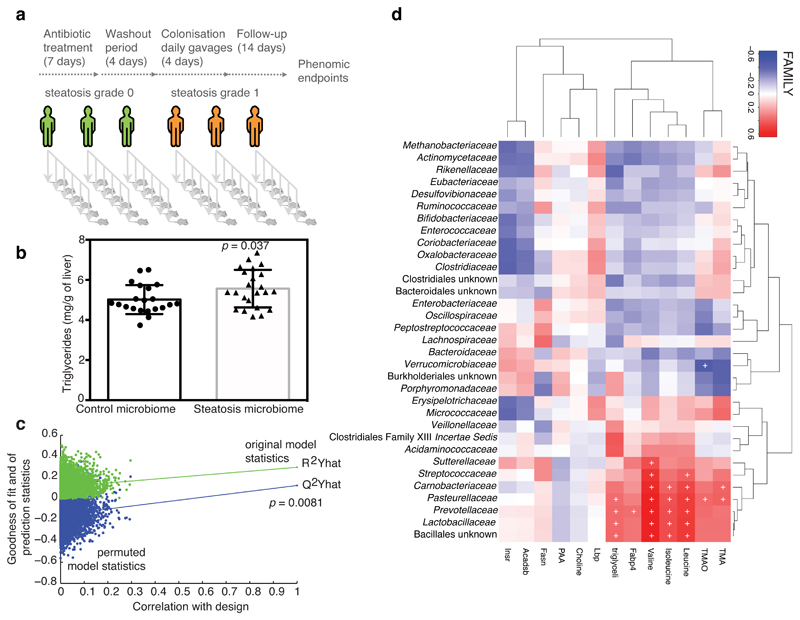
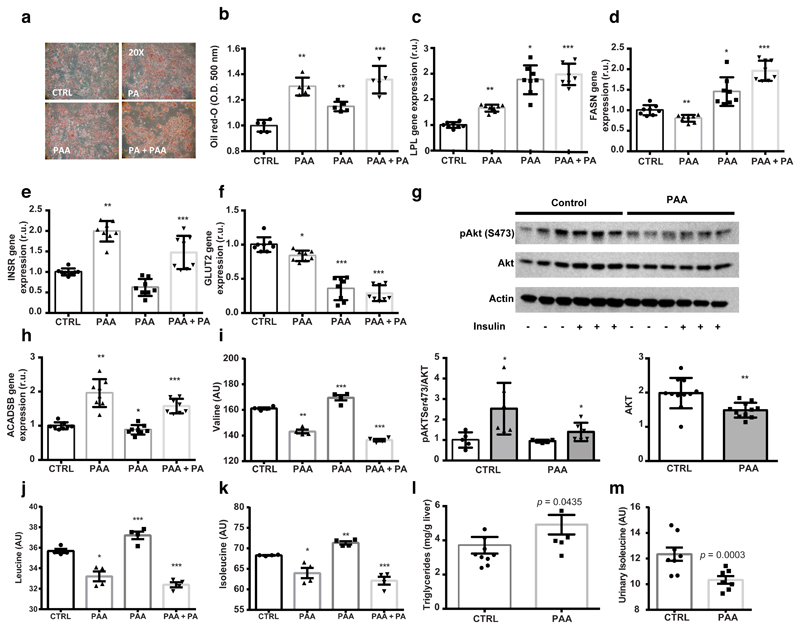
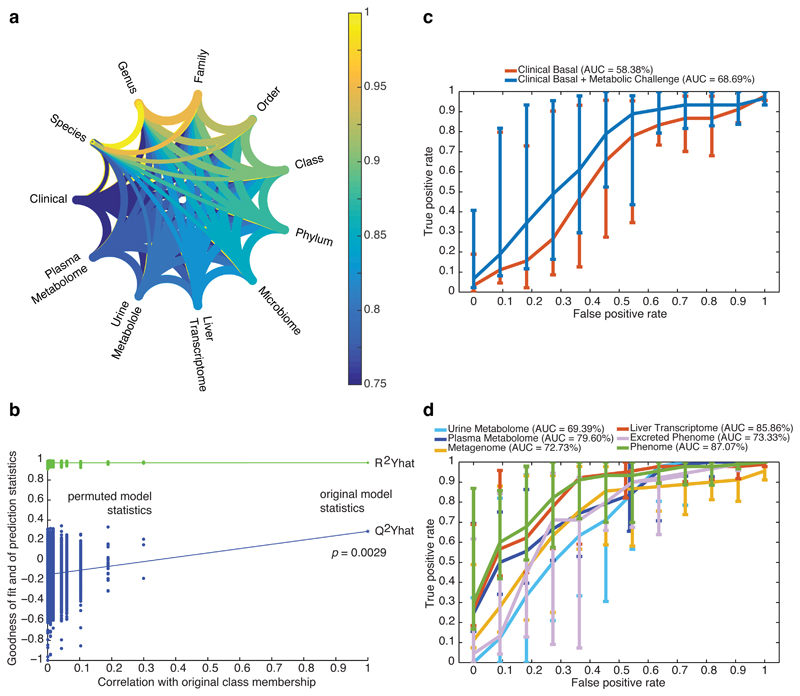
Hepatic steatosis is a multifactorial condition that is often observed in obese patients and is a prelude to non-alcoholic fatty liver disease. Here, we combine shotgun sequencing of fecal metagenomes with molecular phenomics (hepatic transcriptome and plasma and urine metabolomes) in two well-characterized cohorts of morbidly obese women recruited to the FLORINASH study. We reveal molecular networks linking the gut microbiome and the host phenome to hepatic steatosis. Patients with steatosis have low microbial gene richness and increased genetic potential for the processing of dietary lipids and endotoxin biosynthesis (notably from Proteobacteria), hepatic inflammation and dysregulation of aromatic and branched-chain amino acid metabolism. We demonstrated that fecal microbiota transplants and chronic treatment with phenylacetic acid, a microbial product of aromatic amino acid metabolism, successfully trigger steatosis and branched-chain amino acid metabolism. Molecular phenomic signatures were predictive (area under the curve = 87%) and consistent with the gut microbiome having an effect on the steatosis phenome (>75% shared variation) and, therefore, actionable via microbiome-based therapies.
Conflict of interest statement
Figures
Comment in
-
Microbiome metabolomics reveals new drivers of human liver steatosis.Nat Med. 2018 Jul;24(7):906-907. doi: 10.1038/s41591-018-0126-3. Nat Med. 2018. PMID: 29988145 No abstract available.
-
Gut microbiome, microbial metabolites and the development of NAFLD.Nat Rev Gastroenterol Hepatol. 2018 Dec;15(12):719-720. doi: 10.1038/s41575-018-0058-x. Nat Rev Gastroenterol Hepatol. 2018. PMID: 30158571 No abstract available.
References
-
- Saltiel AR, Kahn CR. Insulin signalling and the regulation of glucose and lipid metabolism. Nature. 2001;414:799–806. - PubMed
-
- Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature. 2006;444:840–846. - PubMed
-
- Meex RCR, Watt MJ. Hepatokines: linking nonalcoholic fatty liver disease and insulin resistance. Nat Rev Endocrinol. 2017;13:509–520. - PubMed
-
- Adams LA, Anstee QM, Tilg H, Targher G. Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut. 2017;66:1138–1153. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
