

Evaluation of Dysplasia in Barrett Esophagus
- PMID: 29942221
- PMCID: PMC6009185
Evaluation of Dysplasia in Barrett Esophagus
Abstract
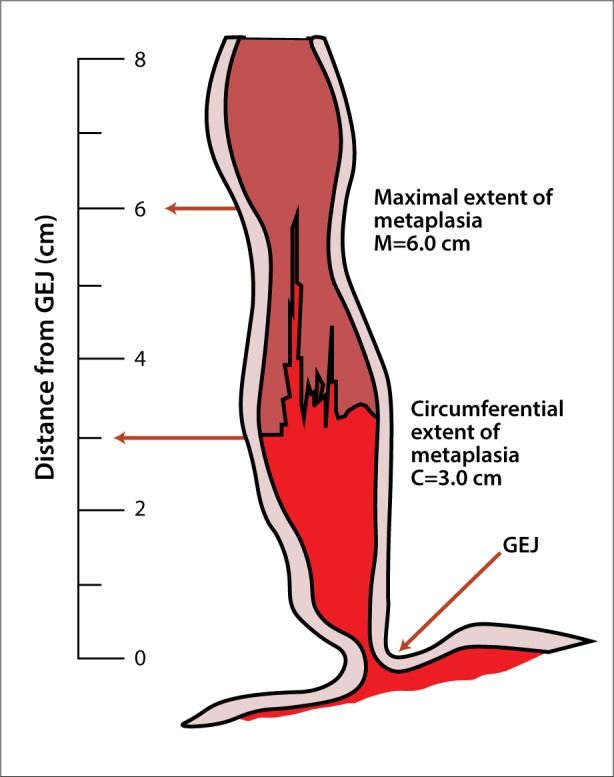
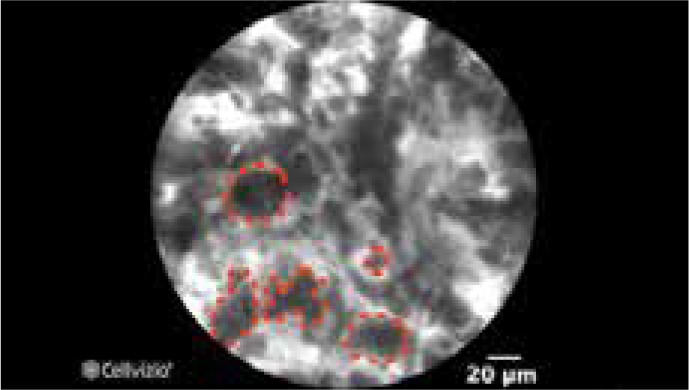
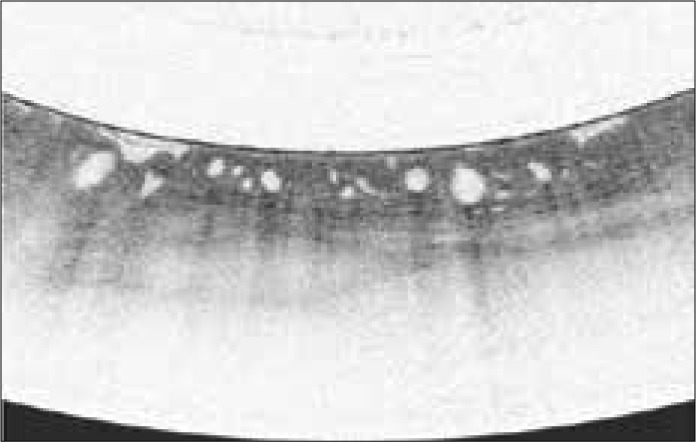
Barrett esophagus (BE) is the precursor lesion to adenocarcinoma of the esophagus. The current surveillance strategy of 4-quadrant Seattle protocol biopsies has been associated with sampling error and missing higher-risk lesions, and there is often less adherence to endoscopic surveillance with long segments. Advancements in endoscopic imaging and sampling techniques allow for better surveillance of BE, particularly when assessing for dysplasia. This article highlights the key endoscopic imaging and sampling advancements in the evaluation of dysplasia in BE.
Keywords: Barrett esophagus; chromoendoscopy; confocal laser endomicroscopy; dysplasia; narrow-band imaging; volumetric laser endomicroscopy.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures

References
-
- Davis-Yadley AH, Neill KG, Malafa MP, Pena LR. Advances in the endoscopic diagnosis of Barrett esophagus. Cancer Control. 2016;23(1):67–77. - PubMed
-
- Evans JA, Early DS, Fukami N, et al. ASGE Standards of Practice Committee; Standards of Practice Committee of the American Society for Gastrointestinal Endoscopy. The role of endoscopy in Barrett’s esophagus and other premalignant conditions of the esophagus. Gastrointest Endosc. 2012;76(6):1087–1094. - PubMed
-
- Ireland CJ, Thompson SK, Laws TA, Esterman A. Risk factors for Barrett’s esophagus: a scoping review. Cancer Causes Control. 2016;27(3):301–323. - PubMed
LinkOut - more resources
Full Text Sources