

Anomalies in T Cell Function Are Associated With Individuals at Risk of Mycobacterium abscessus Complex Infection
- PMID: 29942313
- PMCID: PMC6004551
- DOI: 10.3389/fimmu.2018.01319
Anomalies in T Cell Function Are Associated With Individuals at Risk of Mycobacterium abscessus Complex Infection
Abstract
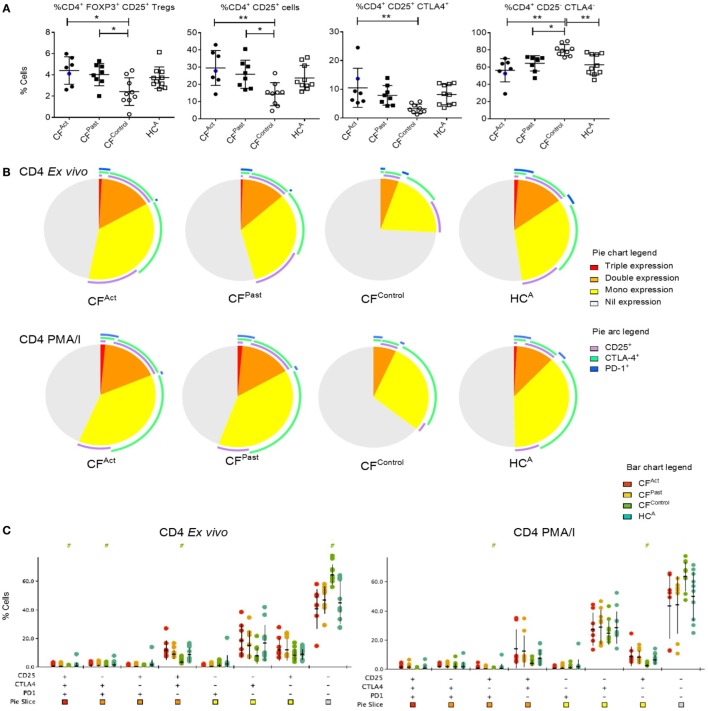
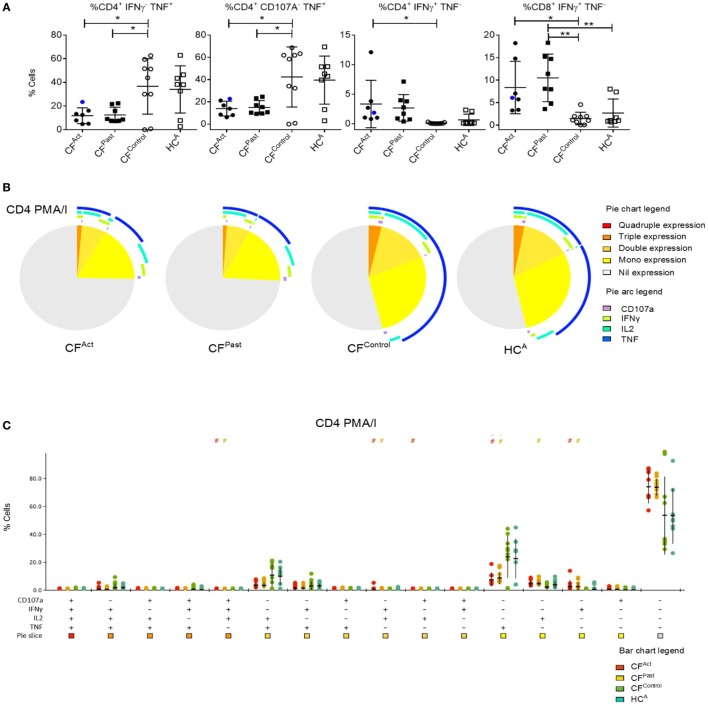
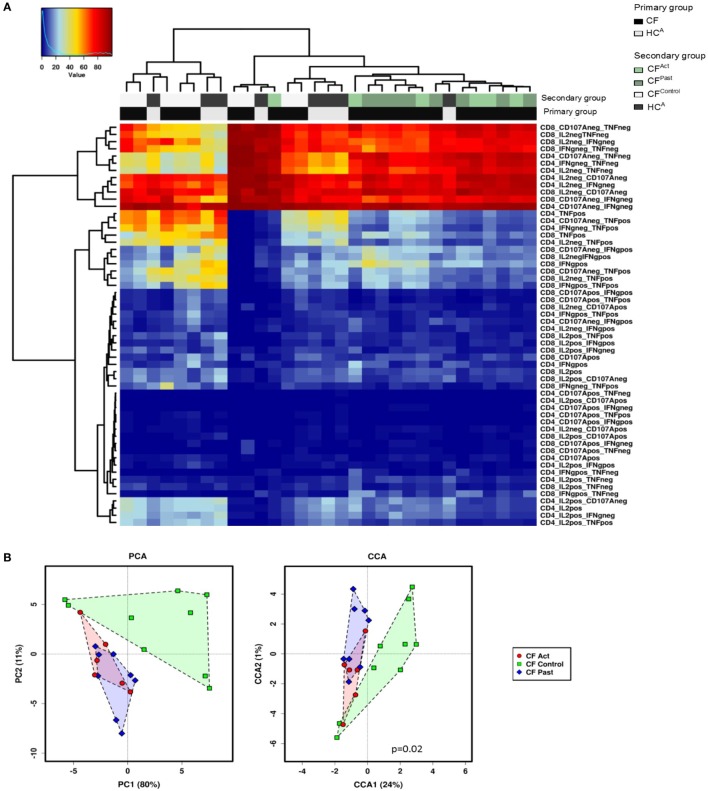
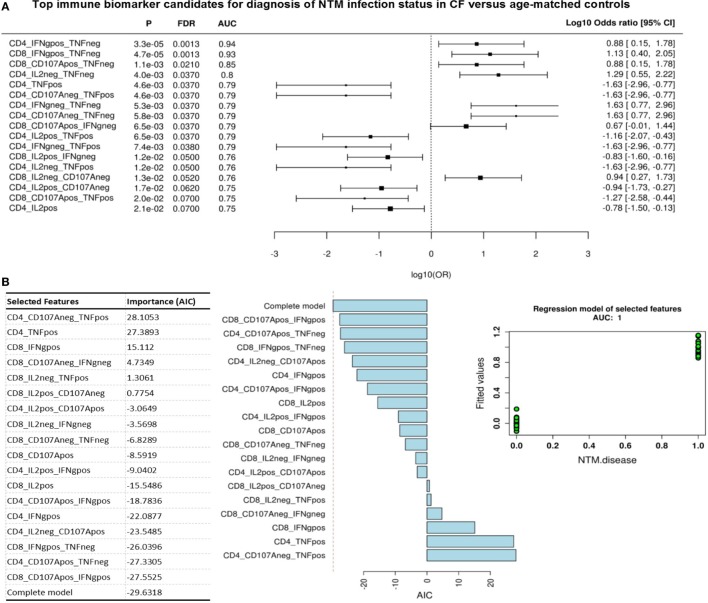
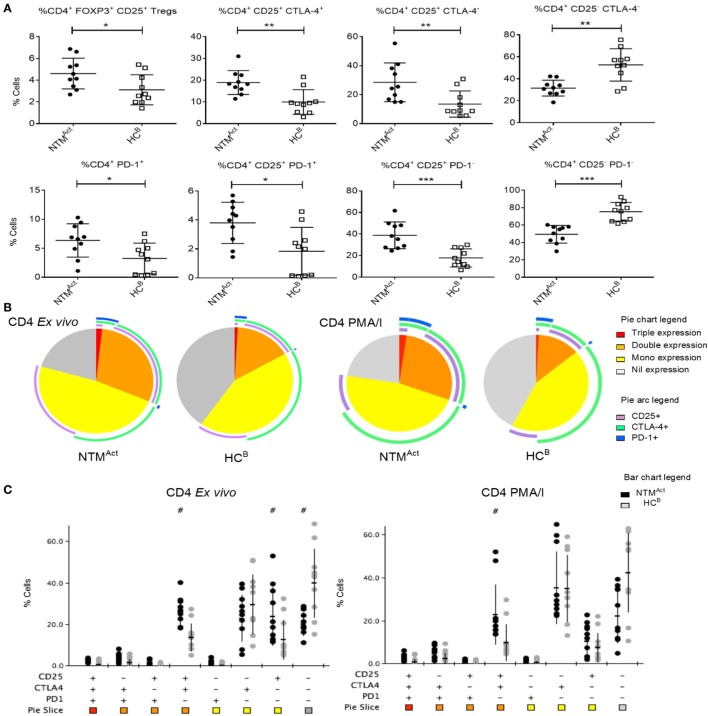
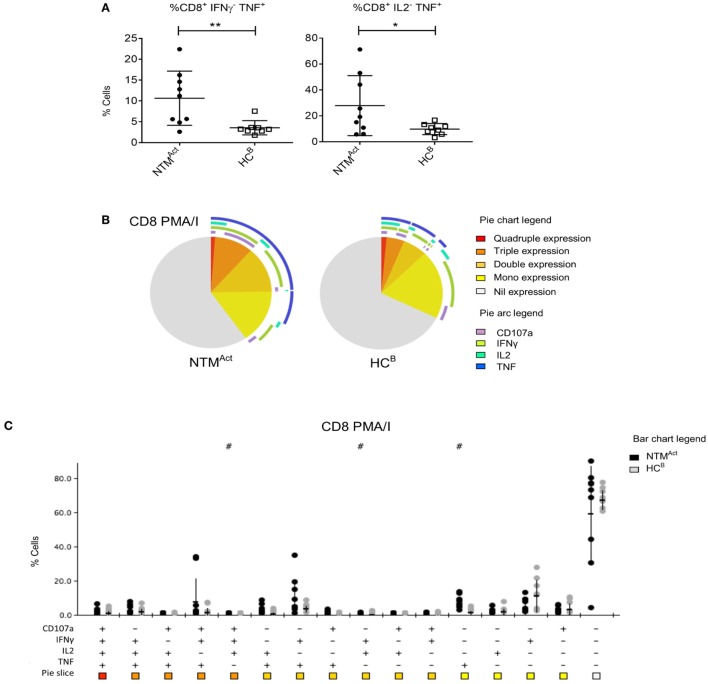
The increasing global incidence and prevalence of non-tuberculous mycobacteria (NTM) infection is of growing concern. New evidence of person-to-person transmission of multidrug-resistant NTM adds to the global concern. The reason why certain individuals are at risk of NTM infections is unknown. Using high definition flow cytometry, we studied the immune profiles of two groups that are at risk of Mycobacterium abscessus complex infection and matched controls. The first group was cystic fibrosis (CF) patients and the second group was elderly individuals. CF individuals with active M. abscessus complex infection or a history of M. abscessus complex infection exhibited a unique surface T cell phenotype with a marked global deficiency in TNFα production during mitogen stimulation. Importantly, immune-based signatures were identified that appeared to predict at baseline the subset of CF individuals who were at risk of M. abscessus complex infection. In contrast, elderly individuals with M. abscessus complex infection exhibited a separate T cell phenotype underlined by the presence of exhaustion markers and dysregulation in type 1 cytokine release during mitogen stimulation. Collectively, these data suggest an association between T cell signatures and individuals at risk of M. abscessus complex infection, however, validation of these immune anomalies as robust biomarkers will require analysis on larger patient cohorts.
Keywords: T cells; cystic fibrosis; immunoprofiling; non-tuberculous mycobacteria; pulmonary non-tuberculous mycobacteria infection.
Figures
Similar articles
-
Clinical and Experimental Determination of Protection Afforded by BCG Vaccination against Infection with Non-Tuberculous Mycobacteria: A Role in Cystic Fibrosis?Vaccines (Basel). 2023 Aug 1;11(8):1313. doi: 10.3390/vaccines11081313. Vaccines (Basel). 2023. PMID: 37631881 Free PMC article.
-
Increasing nontuberculous mycobacteria infection in cystic fibrosis.J Cyst Fibros. 2015 Jan;14(1):53-62. doi: 10.1016/j.jcf.2014.05.008. Epub 2014 Jun 7. J Cyst Fibros. 2015. PMID: 24917112
-
Rapid detection and immune characterization of Mycobacterium abscessus infection in cystic fibrosis patients.PLoS One. 2015 Mar 5;10(3):e0119737. doi: 10.1371/journal.pone.0119737. eCollection 2015. PLoS One. 2015. PMID: 25742660 Free PMC article.
-
Virulence Mechanisms of Mycobacterium abscessus: Current Knowledge and Implications for Vaccine Design.Front Microbiol. 2022 Mar 3;13:842017. doi: 10.3389/fmicb.2022.842017. eCollection 2022. Front Microbiol. 2022. PMID: 35308378 Free PMC article. Review.
-
The Diverse Cellular and Animal Models to Decipher the Physiopathological Traits of Mycobacterium abscessus Infection.Front Cell Infect Microbiol. 2017 Apr 4;7:100. doi: 10.3389/fcimb.2017.00100. eCollection 2017. Front Cell Infect Microbiol. 2017. PMID: 28421165 Free PMC article. Review.
Cited by
-
Characterizing and correcting immune dysfunction in non-tuberculous mycobacterial disease.Front Immunol. 2022 Nov 10;13:1047781. doi: 10.3389/fimmu.2022.1047781. eCollection 2022. Front Immunol. 2022. PMID: 36439147 Free PMC article.
-
Mucosal Immunity in Cystic Fibrosis.J Immunol. 2021 Dec 15;207(12):2901-2912. doi: 10.4049/jimmunol.2100424. J Immunol. 2021. PMID: 35802761 Free PMC article. Review.
-
Innate and Adaptive Lymphocytes in Non-Tuberculous Mycobacteria Lung Disease: A Review.Front Immunol. 2022 Jun 28;13:927049. doi: 10.3389/fimmu.2022.927049. eCollection 2022. Front Immunol. 2022. PMID: 35837393 Free PMC article. Review.
-
Antibiotic Resistance to Mycobacterium tuberculosis and Potential Use of Natural and Biological Products as Alternative Anti-Mycobacterial Agents.Antibiotics (Basel). 2022 Oct 18;11(10):1431. doi: 10.3390/antibiotics11101431. Antibiotics (Basel). 2022. PMID: 36290089 Free PMC article. Review.
-
Non-tuberculous mycobacteria immunopathogenesis: Closer than they appear. a prime of innate immunity trade-off and NTM ways into virulence.Scand J Immunol. 2021 Aug;94(2):e13035. doi: 10.1111/sji.13035. Epub 2021 Jun 22. Scand J Immunol. 2021. PMID: 33655533 Free PMC article. Review.
References
-
- Society TRCotBT. Pulmonary disease caused by Mycobacterium avium-intracellulare in HIV-negative patients: five-year follow-up of patients receiving standardised treatment. Int J Tuberc Lung Dis (2002) 6(7):628–34. - PubMed
-
- Fangous MS, Mougari F, Gouriou S, Calvez E, Raskine L, Cambau E, et al. Classification algorithm for subspecies identification within the Mycobacterium abscessus species, based on matrix-assisted laser desorption ionization-time of flight mass spectrometry. J Clin Microbiol (2014) 52(9):3362–9.10.1128/JCM.00788-14 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources