

Cerebral Oximetry for Detecting High-mortality Risk Patients with Cryptococcal Meningitis
- PMID: 29942819
- PMCID: PMC6007269
- DOI: 10.1093/ofid/ofy105
Cerebral Oximetry for Detecting High-mortality Risk Patients with Cryptococcal Meningitis
Abstract
Background: Cryptococcus is the commonest cause of adult meningitis in Africa, with 50%-70% experiencing increased intracranial pressure. Cerebral oximetry is a noninvasive near-infrared spectroscopy technology to monitor percent regional cerebral tissue oxygenation (rSO2). We assessed if cerebral oximetry predicts meningitis mortality.
Methods: We performed cerebral oximetry within 14 days of cryptococcal meningitis diagnosis on 121 Ugandans from April 2016 to September 2017. We evaluated baseline rSO2 association with mortality by multivariable logistic regression and correlation with other clinical factors. We compared groups formed by initial rSO2 <30% vs ≥30% for longitudinal change with mixed effects models. We measured change in %rSO2 before and after lumbar puncture (LP).
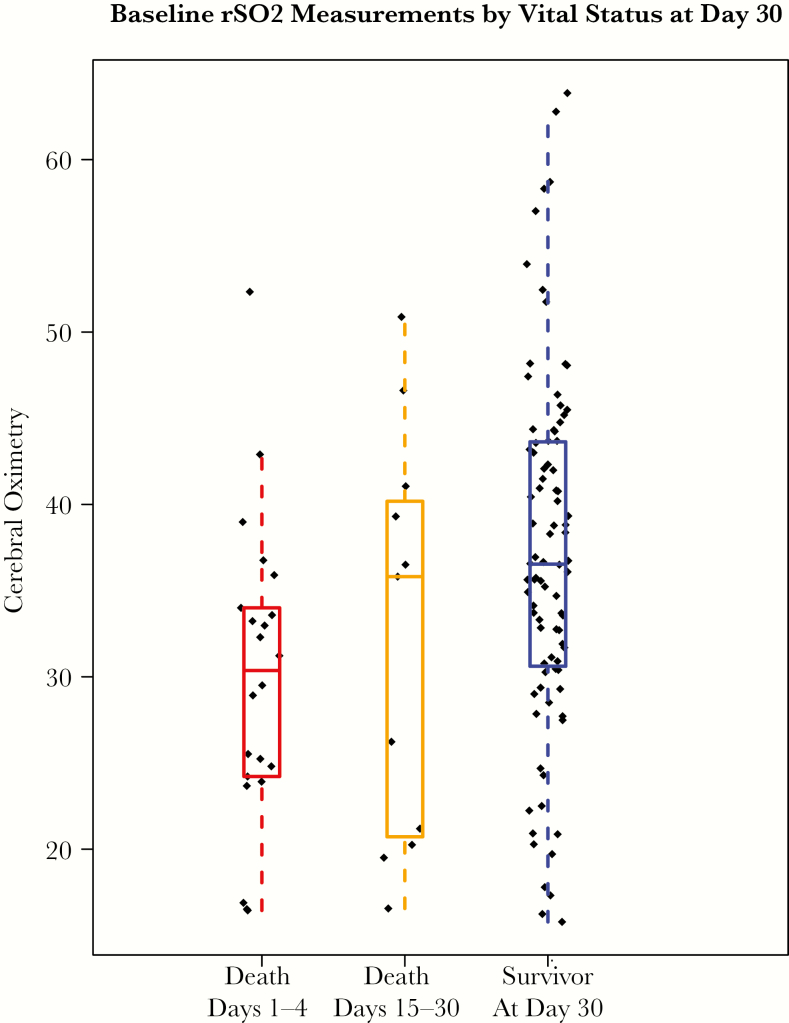
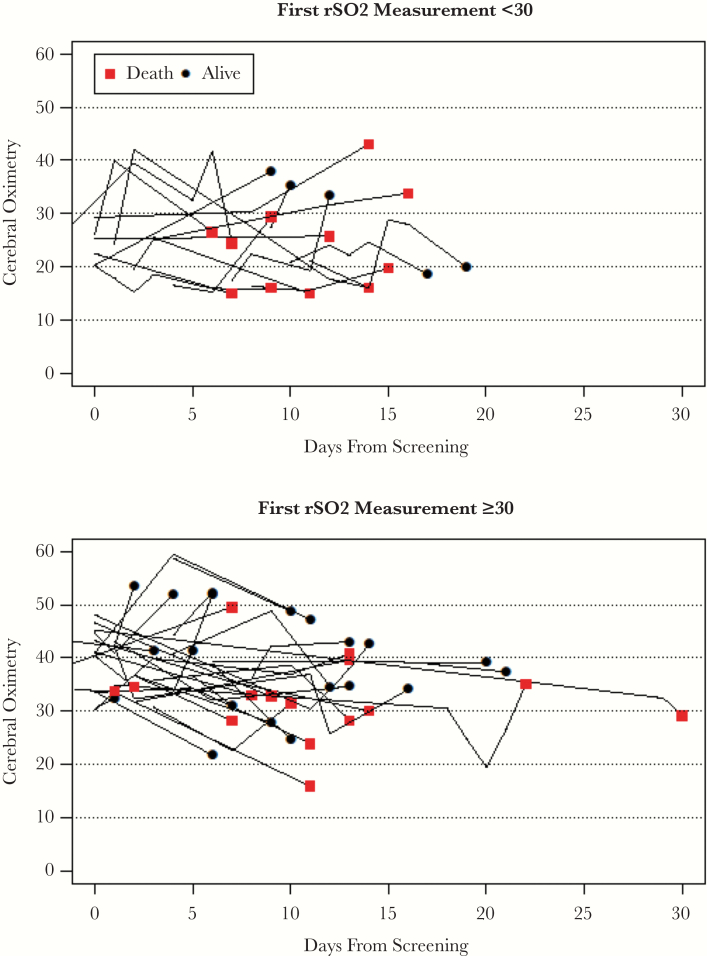
Results: The median initial rSO2 (interquartile range) was 36% (29%-42%), and it was <30% in 29% (35/121). For 30-day mortality, the unadjusted odds ratio (per 5% increase in rSO2) was 0.73 (95% confidence interval [CI], 0.58 to 0.91; P = .005). Those with initial rSO2 <30% had 3.4 (95% CI, 1.5 to 8.0) higher odds of 30-day mortality than those with initial rSO2 ≥30%. Hemoglobin correlated with initial rSO2 (rho = .54; P < .001), but rSO2 did not correlate with pulse oximetry, intracranial pressure, cerebral perfusion pressure, or quantitative cerebrospinal fluid culture, and rSO2 was unchanged pre/post-lumbar punctures. The longitudinal rSO2 measurements change was 15% (95% CI, 12% to 18%) lower in the group with initial rSO2 <30%.
Conclusions: Individuals with cryptococcal meningitis and low cerebral oximetry (rSO2 < 30%) have high mortality. Cerebral oximetry may be useful as a prognostic marker of mortality. Targeted interventions to improve rSO2 should be tested in trials to try to decrease mortality in meningitis.
Keywords: cerebrovascular circulation; cryptococcal meningitis; hemodynamic monitoring; mortality; oximetry; physiologic monitoring.
Figures
References
-
- Graybill JR, Sobel J, Saag M, et al. . Diagnosis and management of increased intracranial pressure in patients with AIDS and cryptococcal meningitis. The NIAID Mycoses Study Group and AIDS Cooperative Treatment Groups. Clin Infect Dis 2000; 30:47–54. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
