

Severe Cushing Syndrome Due to an ACTH-Producing Pheochromocytoma: A Case Presentation and Review of the Literature
- PMID: 29942926
- PMCID: PMC6007244
- DOI: 10.1210/js.2018-00086
Severe Cushing Syndrome Due to an ACTH-Producing Pheochromocytoma: A Case Presentation and Review of the Literature
Abstract
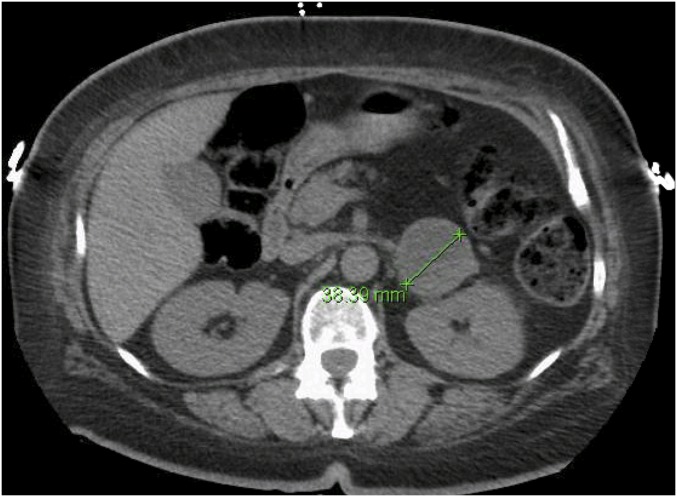
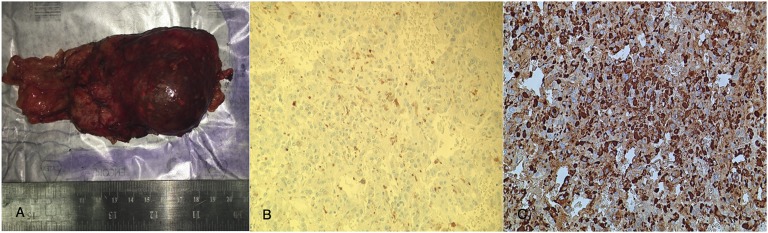
Adrenocorticotropic hormone (ACTH)-dependent Cushing syndrome is rarely caused by a pheochromocytoma. We present a case of a 46-year-old woman who developed severe hypertension, hypokalemia, and typical Cushingoid features. Investigations revealed extremely high metanephrine, cortisol, and ACTH levels. Imaging showed a 3.8-cm left adrenal mass. Preoperative control of hypertension and hypokalemia was very challenging. The patient was cured after surgical removal of the adrenal mass. We followed this by a review of the literature using the databases Google Scholar and PubMed. A total of 58 cases have been reported to date. In summary, ACTH-producing pheochromocytoma is a rare condition that poses a clinical challenge in the perioperative period. It is important that physicians be aware of such a condition because early recognition and treatment are crucial to decrease morbidity and mortality.
Keywords: ACTH-producing pheochromocytoma; Cushing syndrome; ectopic; pheochromocytoma.
Figures
References
-
- Newell-Price J, Bertagna X, Grossman AB, Nieman LK. Cushing’s syndrome. Lancet. 2006;367(9522):1605–1617. - PubMed
-
- Lindholm J, Juul S, Jørgensen JO, Astrup J, Bjerre P, Feldt-Rasmussen U, Hagen C, Jørgensen J, Kosteljanetz M, Kristensen L, Laurberg P, Schmidt K, Weeke J. Incidence and late prognosis of cushing’s syndrome: a population-based study. J Clin Endocrinol Metab. 2001;86(1):117–123. - PubMed
-
- Etxabe J, Vazquez JA. Morbidity and mortality in Cushing’s disease: an epidemiological approach. Clin Endocrinol (Oxf). 1994;40(4):479–484. - PubMed
-
- Ballav C, Naziat A, Mihai R, Karavitaki N, Ansorge O, Grossman AB. Mini-review: pheochromocytomas causing the ectopic ACTH syndrome. Endocrine. 2012;42(1):69–73. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources