

Long-term effects of device-guided slow breathing in stable heart failure patients with reduced ejection fraction
- PMID: 29943271
- PMCID: PMC6333716
- DOI: 10.1007/s00392-018-1310-7
Long-term effects of device-guided slow breathing in stable heart failure patients with reduced ejection fraction
Abstract
Background: Slow breathing (SLOWB) alleviates symptoms of chronic heart failure (HF) but its long-term effects are unknown. We examined the acute and long-term impact of device-guided breathing on hemodynamics and prognostic parameters in HF patients with reduced ejection fraction (HFrEF).
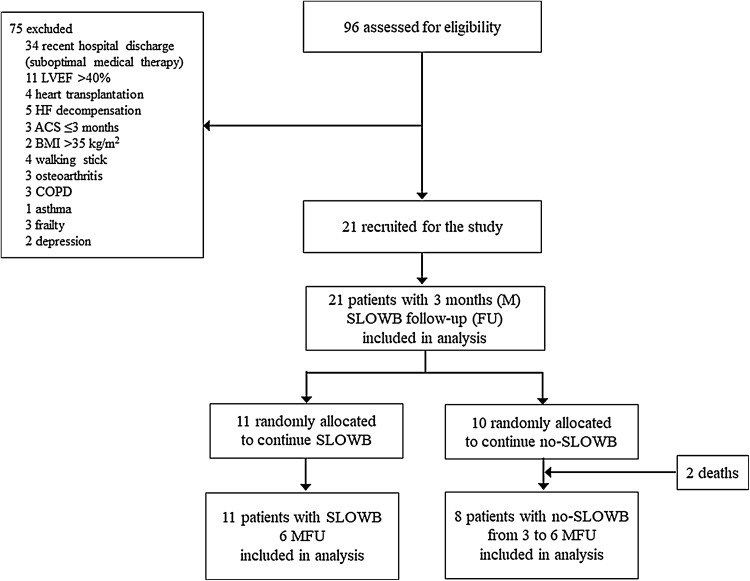
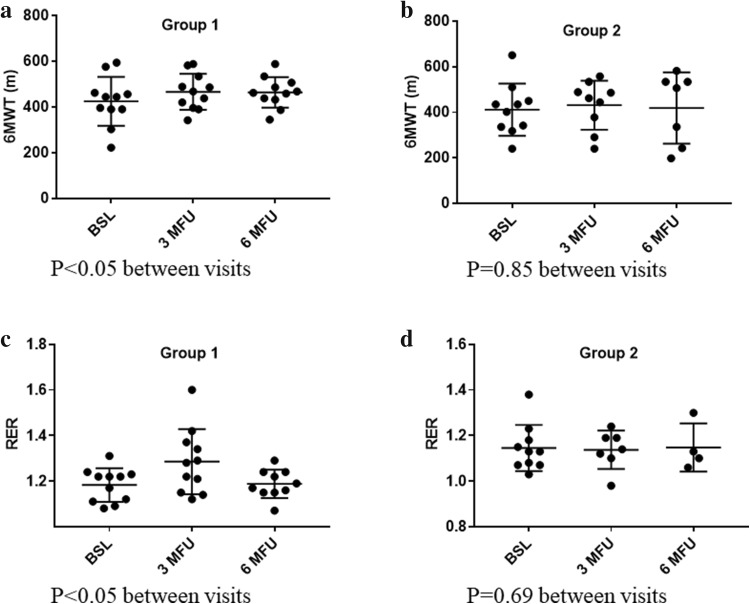
Methods and results: Twenty-one patients with HFrEF (23.9 ± 5.8%, SD ± mean) on optimal medical therapy underwent blood pressure (BP), heart rate (HR), HR variability, 6-min walk test (6MWT), cardiopulmonary exercise testing (CPET), and echocardiography measurements before and 3 months after SLOWB home training (30 min daily). After 3 months, all patients were assigned to continue SLOWB (Group 1) or no-SLOWB (Group 2). All tests were repeated after 6 months. Acute SLOWB (18 ± 5 vs 8 ± 2 breaths/min, P < 0.001) had no influence on BP and HR but improved saturation (97 ± 2 vs 98 ± 2%, P = 0.01). Long-term SLOWB reduced office systolic BP (P < 0.001) but not central or ambulatory systolic BP. SLOWB reduced SDNN/RMSSD ratio (P < 0.05) after 3 months. One-way repeated measures of ANOVA revealed a significant increase in 6MWT and peak RER (respiratory exchange ratio) from baseline to 6-month follow-up in group 1 (P < 0.05) but not group 2 (P = 0.85 for 6MWT, P = 0.69 for RER). No significant changes in echocardiography were noted at follow-up. No HF worsening, rehospitalisation or death occurred in group 1 out to 6-month follow-up. Two hospitalizations for HF decompensation and two deaths ensued in group 2 between 3- and 6-month follow-up.
Conclusions: SLOWB training improves cardiorespiratory capacity and appears to slow the progression of HFrEF. Further long-term outcome studies are required to confirm the benefits of paced breathing in HFrEF.
Keywords: 6-Min walk test; Functional capacity; Heart failure with reduced ejection fraction; Heart rate variability; Hemodynamics; Slow breathing.
Conflict of interest statement
All the authors declare that they have no competing interests.
Figures
References
-
- Krone M, Dufner V, Wagner M, Gelbrich G, Ertl G, Heuschmann PU. Public funding for medical research in relation to the burden of disease caused by cardiovascular diseases and neoplasms in Germany. Clin Res Cardiol. 2018 - PubMed
-
- Kirchhof G, Lindner JF, Achenbach S, Berger K, Blankenberg S, Fangerau H, Gimpel H, Gassner UM, Kersten J, Magnus D, Rebscher H, Schunkert H, Rixen S, Kirchhof P. Stratified prevention: opportunities and limitations. Report on the 1st interdisciplinary cardiovascular workshop in Augsburg. Clin Res Cardiol. 2018;107(3):193–200. doi: 10.1007/s00392-017-1186-y. - DOI - PMC - PubMed
-
- Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, Chiuve SE, Cushman M, Delling FN, Deo R, de Ferranti SD, Ferguson JF, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Lutsey PL, Mackey JS, Matchar DB, Matsushita K, Mussolino ME, Nasir K, O’Flaherty M, Palaniappan LP, Pandey A, Pandey DK, Reeves MJ, Ritchey MD, Rodriguez CJ, Roth GA, Rosamond WD, Sampson UKA, Satou GM, Shah SH, Spartano NL, Tirschwell DL, Tsao CW, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Council on E, Prevention Statistics C, Stroke Statistics S Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. 2018;137(12):e67–e492. doi: 10.1161/CIR.0000000000000558. - DOI - PubMed
-
- Tschope C, Birner C, Bohm M, Bruder O, Frantz S, Luchner A, Maier L, Stork S, Kherad B, Laufs U. Heart failure with preserved ejection fraction: current management and future strategies: expert opinion on the behalf of the Nucleus of the “Heart Failure Working Group” of the German Society of Cardiology (DKG) Clin Res Cardiol. 2018;107(1):1–19. doi: 10.1007/s00392-017-1170-6. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
