

Detection of MRSA in nasal swabs-marked reduction of time to report for negative reports by substituting classical manual workflow with total lab automation
- PMID: 29943308
- PMCID: PMC6133036
- DOI: 10.1007/s10096-018-3308-5
Detection of MRSA in nasal swabs-marked reduction of time to report for negative reports by substituting classical manual workflow with total lab automation
Abstract
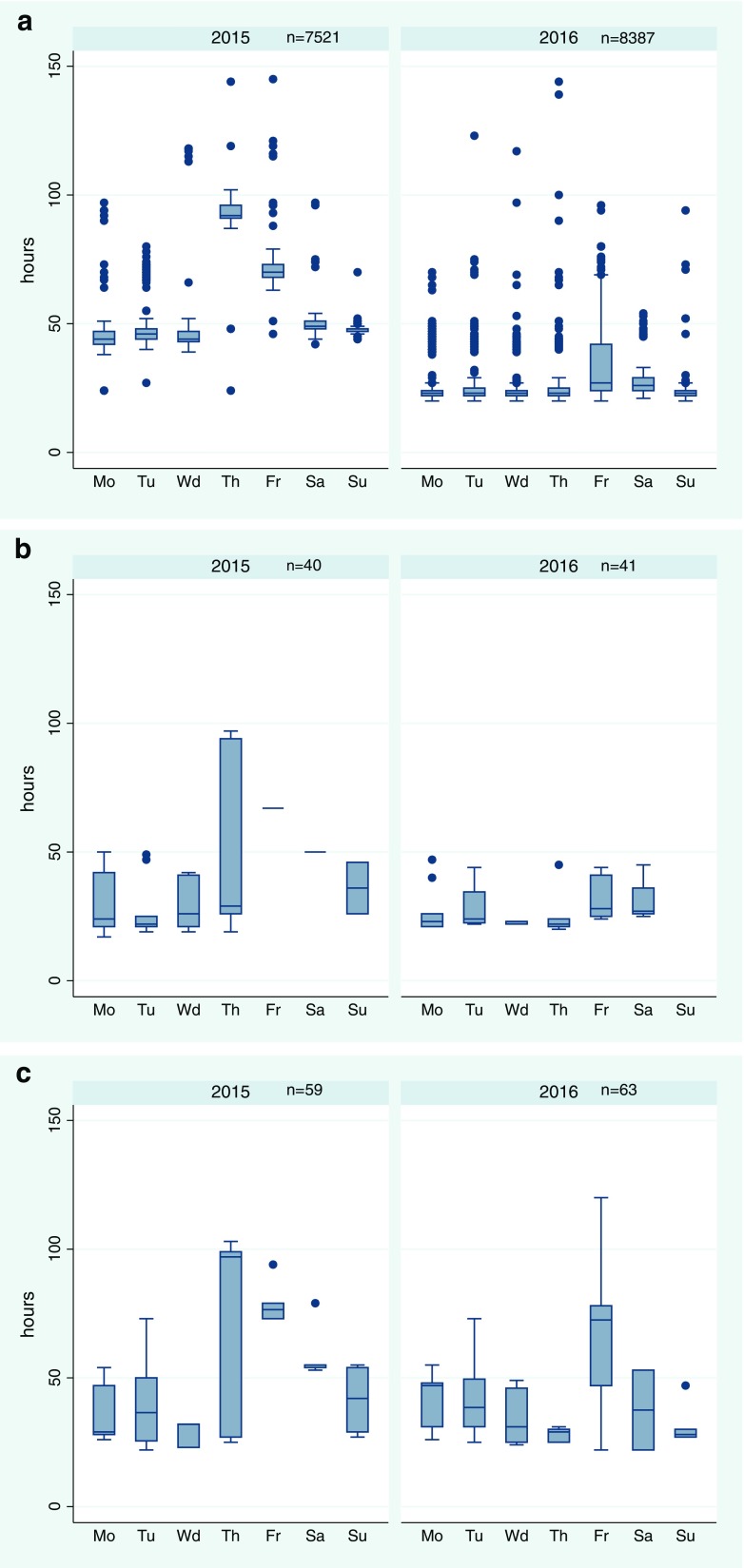
In 2016, the workflow for MRSA detection in nasal swabs was changed from a classic-manual workflow to an automated workflow using total lab automation (TLA; BD Kiestra). This change entailed a reduction of the incubation time from 2 days to 20 h and reading of plates on weekdays and weekends instead of weekdays only. The workflow alteration did not include the introduction of 24/7. We wanted to follow up on the consequences for the times to report (TTR). We compared the TTR of all nasal swabs, which were sent for MRSA detection from June until August in 2015 (workflow-classic-manual) and in 2016 (workflow-automated). We calculated median TTR and interquartile ranges for the three possible reporting outcomes (negative, MRSA-known, MRSA-new) per day and workflow. A multivariable linear regression modeled the exposure variables workflow, day, and reporting outcome on TTR including interaction variables. The quantity and reasons for a TTR longer than 3 days were analyzed. During both 3-month periods, a total of 16,111 reports were issued (2015:7620; 2016:8491). The median TTR for negative reports was 48:28 (hh:mm) in 2015 and 23:58 in 2016. In the linear regression, all exposure variables had a strong and highly significant (p < 0.001) influence on the TTR. The number of reports with a TTR longer than 3 days shrank from 2418 (2015) to 60 (2016). The workflow alteration halved the median TTR for negative reports and the number of reports with a TTR longer than 3 days was reduced by 97.5%.
Keywords: Automation; MRSA; Time to result; Workflow.
Conflict of interest statement
Conflict of interest
IB has received speaker honoraria from Becton Dickinson; SH, none, FB, none; and SZ has received speaker honoraria from Becton Dickinson.
Ethical approval
For this type of study, formal consent is not required.
Informed consent
Not applicable
Figures
References
-
- Humphreys H, Becker K, Dohmen PM, Petrosillo N, Spencer M, van Rijen M, Wechsler-Fordos A, Pujol M, Dubouix A, Garau J. Staphylococcus aureus and surgical site infections: benefits of screening and decolonization before surgery. J Hosp Infect. 2016;94(3):295–304. doi: 10.1016/j.jhin.2016.06.011. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
