

Impact of Providing Preexposure Prophylaxis for Human Immunodeficiency Virus at Clinics for Sexually Transmitted Infections in Baltimore City: An Agent-based Model
- PMID: 29944642
- PMCID: PMC6339460
- DOI: 10.1097/OLQ.0000000000000882
Impact of Providing Preexposure Prophylaxis for Human Immunodeficiency Virus at Clinics for Sexually Transmitted Infections in Baltimore City: An Agent-based Model
Abstract
Background: Preexposure prophylaxis (PrEP) greatly reduces the risk of human immunodeficiency virus (HIV) acquisition, but its optimal delivery strategy remains uncertain. Clinics for sexually transmitted infections (STIs) can provide an efficient venue for PrEP delivery.
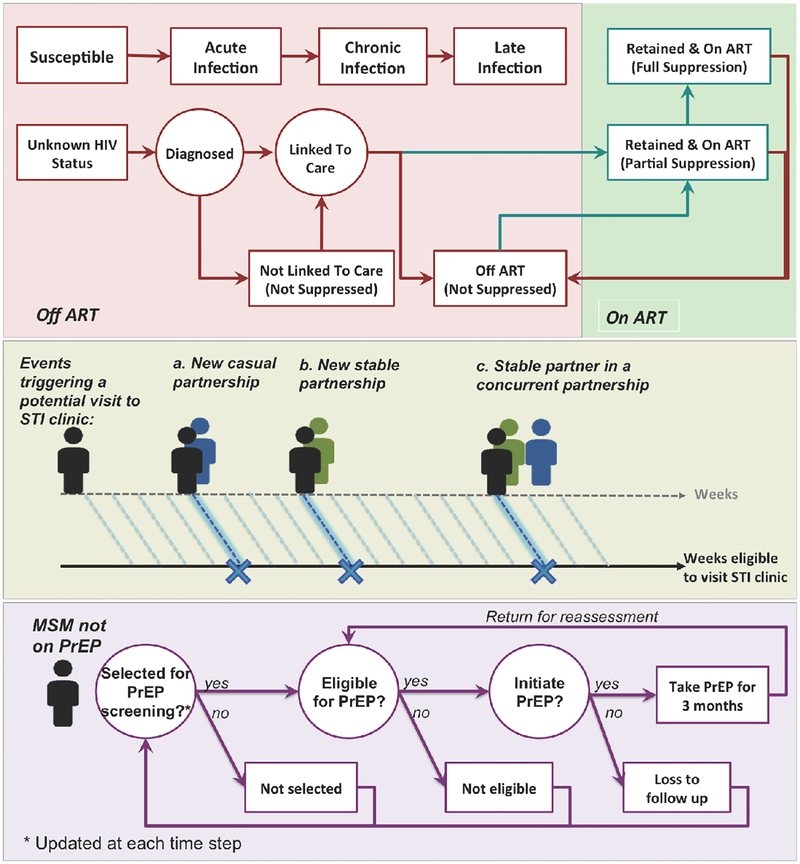
Methods: To quantify the added value of STI clinic-based PrEP delivery, we used an agent-based simulation of HIV transmission among men who have sex with men (MSM). We simulated the impact of PrEP delivery through STI clinics compared with PrEP delivery in other community-based settings. Our primary outcome was the projected 20-year reduction in HIV incidence among MSM.
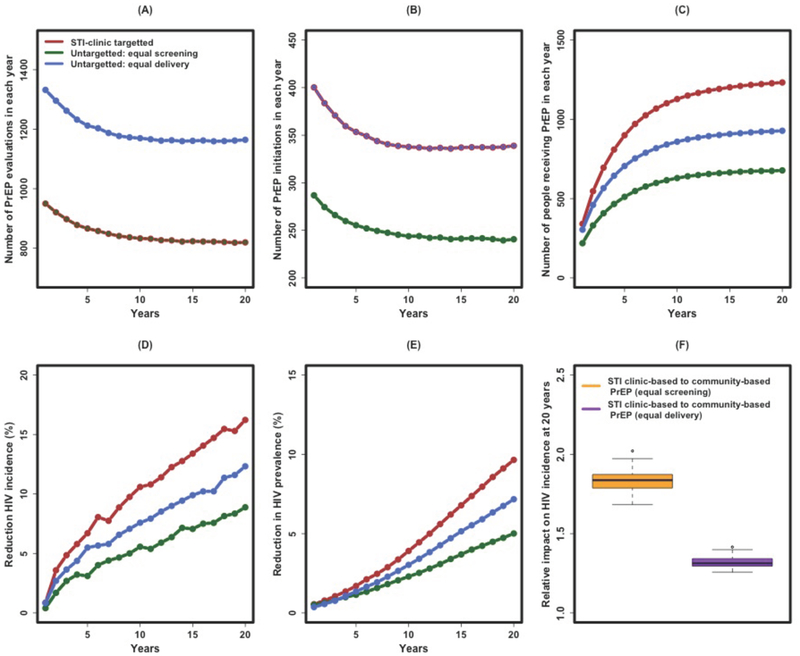
Results: Assuming PrEP uptake and adherence of 60% each, evaluating STI clinic attendees and delivering PrEP to eligible MSM reduced HIV incidence by 16% [95% uncertainty range, 14%-18%] over 20 years, an impact that was 1.8 (1.7-2.0) times as great as that achieved by evaluating an equal number of MSM recruited from the community. Comparing strategies where an equal number of MSM received PrEP in each strategy (ie, evaluating more individuals for PrEP in the community-based strategy, because MSM attending STI clinics are more likely to be PrEP eligible), the reduction in HIV incidence under the STI clinic-based strategy was 1.3 (1.3-1.4) times as great as that of community-based delivery.
Conclusions: Delivering PrEP to MSM who attend STI clinics can improve efficiency and effectiveness. If high levels of adherence can be achieved in this population, STI clinics may be an important venue for PrEP implementation.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention. Diagnoses of HIV Infection in the United States and Dependent Areas, 2015. HIV Surveill Rep. 2015;27.
-
- Centers for Disease Control Prevention. HIV Among Gay and Bisexual Men [Internet]. 2015. Available from: http://www.cdc.gov/hiv/group/msm/
-
- Centers for Disease Control Prevention. Preexposure Prophylaxis for the Prevention of HIV Infection in the United States – 2014 Clinical Practice Guideline. 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
